2023.06 OIG Memorandum 23-085.pdf
Unknown Volume 128 pages 6 redactions 0.0% redacted
Help categorize this page (click to add/remove your vote)
1 redactions
1 redactions
1 redactions
1 redactions
2 redactions
LIMITED OFFICIAL USE - PROPRIETARY INFORMATION Investigation and Review of the Federal Bureau of Prisons’ Custody, Care, and Supervision of Jeffrey Epstein at the Metropolitan Correctional Center in New York, New York I N V E S T I G AT I O N S D I V I S I O N 2 3 - 0 8 5 JUNE 2023 * * *
HEADER TEXT GOES HERE i E X E C U T I V E S U M M A R Y Investigation and Review of the Federal Bureau of Prisons’ Custody, Care, and Supervision of Jeffrey Epstein at the Metropolitan Correctional Center in New York, New York Introduction and Background According to its website, the Federal Bureau of Prisons (BOP)’s current mission statement is “Corrections professionals who foster a humane and secure environment and ensure public safety by preparing individuals for successful reentry into our communities.” However, the Department of Justice (DOJ) Office of the Inspector General (OIG) has repeatedly identified long-standing operational challenges that negatively affect the BOP’s ability to operate its institutions safely and securely. Many of those same operational challenges, including staffing shortages, managing inmates at risk for suicide, functional security camera systems, and management failures and widespread disregard of BOP policies and procedures, were again identified by the OIG during this investigation and review into the custody, care, and supervision of one of the BOP’s most notorious inmates, Jeffrey Epstein. The OIG initiated this investigation upon receipt of information from the BOP that on August 10, 2019, in the Metropolitan Correctional Center in New York, New York (MCC New York), Epstein was found hanged in his assigned cell within the Special Housing Unit (SHU). The Office of the Chief Medical Examiner, City of New York, determined that Epstein had died by suicide. The OIG conducted this investigation jointly with the Federal Bureau of Investigation (FBI), with the OIG’s investigative focus being the conduct of BOP personnel. Among other things, the FBI investigated the cause of Epstein’s death and determined there was no criminality pertaining to how Epstein had died. This report concerns the OIG’s findings regarding MCC New York personnel’s custody, care, and supervision of Epstein while...
i i ii psychological observation, for inmates who are stabilizing but not yet ready to return to a housing unit. Epstein was removed from suicide watch on July 24 but remained under psychological observation until July 30. Epstein first told MCC New York staff he thought his cellmate had tried to kill him, but later said he did not know what occurred and did not want to talk about how he had sustained his injuries. Epstein also later asked if he could be housed with the same cellmate. Another inmate housed on the same SHU tier told the OIG that he heard Epstein’s cellmate call for assistance, and that Epstein’s cellmate told him that Epstein tried to hang himself from the bunkbed ladder. Disciplinary charges against Epstein for alleged self-mutilation were not sustained due to insufficient evidence. Following the July 23 incident, the Psychology Department determined Epstein needed to be housed with an appropriate cellmate, and on July 30 it sent an email to over 70 MCC New York employees informing them of this requirement. The Warden at the time told the OIG that he selected a new cellmate for Epstein in consultation with BOP executive leadership. That inmate remained Epstein’s cellmate until August 9. Events of August 8–10, 2019, and Epstein’s Death On August 8, the U.S. Marshals Service sent two emails notifying numerous MCC New York staff that Epstein’s cellmate was being transferred to another facility on August 9. However, no action was taken to ensure Epstein was assigned another cellmate. Also on August 8, Epstein met with his attorneys at the prison, as he had on prior occasions, and signed a new Last Will and Testament. MCC New York officials did not learn about the new Will until after Epstein’s death. The following day, August 9, Epstein’s cellmate was transferred to another facility and he was not assigned a new cellmate. Additionally, on that date, the U.S. Court of Appeals for the Second Circuit unseale...
iii cause of death was hanging and the manner of death was suicide. Blood toxicology tests did not reveal any medications or illegal substances in Epstein’s system. The Medical Examiner who performed the autopsy told the OIG that Epstein’s injuries were consistent with suicide by hanging and that there was no evidence of defensive wounds that would be expected if his death had been a homicide. Epstein did not have marks on his hands, broken fingernails or debris under them, contusions to his knuckles that would have evidenced a fight, or, other than an abrasion on his arm likely due to convulsing from hanging, bruising on his body. The Limited Available Video Evidence Recorded video evidence for August 9 and 10 for the SHU area where Epstein was housed was only available from one prison security camera due to a malfunction of MCC New York’s Digital Video Recorder system that occurred on July 29, 2019. While the prison’s cameras continued to provide live video feeds, recordings were made for only about half the cameras. MCC New York personnel discovered this failure on August 8, 2019, but it was not repaired until after Epstein’s death. As detailed in this report, like many other BOP facilities, MCC New York had a history of security camera problems. The available recorded video footage from the one SHU camera captured a large part of the common area of the SHU and portions of the stairways leading to the different SHU tiers, including Epstein’s cell tier. Thus, anyone entering or attempting to enter Epstein’s SHU tier from the SHU common area would have been picked up by that video camera. Epstein’s cell door, however, was not in the camera’s field of view. The OIG reviewed the video and found that, between approximately 10:40 p.m. on August 9 and about 6:30 a.m. on August 10, no one was seen entering Epstein’s cell tier from the SHU common area. The OIG determined that movements captured on video before and after t...
iv SHU staff told the OIG that at approximately 8 p.m. on August 9, all SHU inmates, including Epstein, were locked in their cells for the evening and we found no evidence to the contrary. The prison’s recorded video did not identify any staff or other individuals approaching Epstein’s SHU tier from the SHU common area between approximately 10:40 p.m. on August 9 and about 6:30 a.m. on August 10. Additionally, the OIG did not observe on the recorded video that Noel and Thomas, who were seated at the desk at the SHU Officers’ Station immediately outside the area where Epstein was housed, at any time during the time period rose from their seats or approached the cell block. We additionally found that Thomas’s and Noel’s reaction on the morning of August 10 upon finding Epstein hanging in his cell, as described to us by Thomas, Noel, the responding Lieutenant, and inmates, was consistent with their being unaware of any potential harm to Epstein prior to Thomas entering Epstein’s cell at about 6:30 a.m. on August 10. None of the MCC New York staff members we interviewed were aware of any information suggesting Epstein’s cause of death was something other than suicide. Additionally, none of the inmates we interviewed had any credible information suggesting Epstein’s cause of death was something other than suicide. Further, the SHU staff and three interviewed inmates with a direct line of sight to Epstein’s cell door on the night of his death stated that no one entered or exited Epstein’s cell after the SHU staff returned Epstein to his cell on August 9. As noted, the surveillance camera in the SHU area where Epstein was housed was live streaming movement in the hallway outside of Epstein’s cell. Although the camera was not recording the captured video, the camera was in plain view of the inmates and therefore inmates would have been aware that any hallway movements, including into or out of Epstein’s cell, could be monitored...
Table of Contents Chapter 1: Introduction .................................................................................................................................. 1 Chapter 2: Background ................................................................................................................................... 5 I. Significant Entities and Individuals ...................................................................................................................5 II. Methodology ................................................................................................................................................6 III. Applicable Law, Regulations, and BOP Policies .......................................................................................7 A. Standards of Conduct .............................................................................................................................7 B. False Statements and Lack of Candor ..................................................................................................8 C. Relevant BOP Policies Regarding the Operation of Correctional Facilities .....................................8 Chapter 3: Timeline of Key Events ............................................................................................................... 14 Chapter 4: Custody and Care of Epstein Prior to His Death ...................................................................... 21 I. Epstein’s Arrest and Detention on July 6 ...................................................................................................... 21 II. MCC New York’s Special Housing Unit ................................................................................................... 22 III. Epstein’s Initial Cell and Cellmate Assignment from July 7 to July 23 ................................................ 28 IV. Events of July 23 and the Placement of Epstein on Suicide Watch an...
A. SHU Inmate Counts.............................................................................................................................. 61 B. Staff Rounds in the SHU ...................................................................................................................... 67 VI. Epstein’s Death on August 10 ................................................................................................................. 70 A. Discovery of Epstein Hanged in Cell and Emergency Response .................................................... 70 B. Items Found in Epstein’s Cell on August 10 Following His Death .................................................. 76 C. Autopsy Results .................................................................................................................................... 79 Chapter 6: The Availability of Limited Recorded Video Evidence Due to the Security Camera Recording System Failure .............................................................................................................................. 81 I. Background on the Security Camera System at MCC New York ............................................................... 81 II. Discovery of Security Camera System Recording Issues in August 2019 .......................................... 82 A. Discovery on August 8 of the DVR 2 Failure that Occurred on July 29 .......................................... 82 B. Response on August 8 and 9 to Discovery of the Recording Failure ............................................ 83 C. SHU Camera Locations and Operational Status on August 10 ...................................................... 84 D. FBI Forensic Analysis of the DVR System .......................................................................................... 92 Chapter 7: Conclusions and Recommendations ......................................................................................... 94 I. Concl...
1 Chapter 1: Introduction The Federal Bureau of Prisons (BOP) is a component of the Department of Justice (DOJ) that operates 122 institutions across the United States. According to its website, the BOP’s current mission statement is “Corrections professionals who foster a humane and secure environment and ensure public safety by preparing individuals for successful reentry into our communities.” However, the DOJ Office of the Inspector General (OIG) has issued numerous reports over more than a decade identifying long-standing operational challenges facing the BOP that have negatively affected its ability to operate its institutions safely and securely. Those reports have contained dozens of recommendations to the BOP. As we detail in this report, many of those same operational challenges and systemic issues, including significant staffing shortages, providing appropriate custody and care of inmates at risk for suicide, the absence of functional security camera systems, and management failures and widespread disregard of BOP policies and procedures, were once again identified by the OIG during the course of this investigation and review into the custody, care, and supervision of one of the BOP’s most notorious inmates, Jeffrey Epstein. We therefore make further recommendations to the BOP in the conclusion of this report to help it address these recurring issues. The OIG initiated this investigation upon the receipt of information from the BOP that on the morning of August 10, 2019, in the Metropolitan Correctional Center located in New York, New York (MCC New York), inmate Jeffery Epstein was found hanged in his assigned cell within the Special Housing Unit (SHU). The SHU is a housing unit where inmates are securely separated from the general inmate population and kept locked in their cells for approximately 23 hours a day, to ensure their own safety as well as the safety of staff and other inmates. Epstein had been placed in the SHU...
2 moved by medical staff to the MCC New York Health Service Unit.1 The Clinical Nurse continuously administered CPR until he was relieved by outside Emergency Medical Technicians (EMT) when they arrived at the Health Services Area minutes later. The EMTs continued CPR, intubated Epstein, and administered medication and fluids in their efforts to revive him. At approximately 7:10 a.m., Epstein was transported by the EMTs in an ambulance to New York Presbyterian Lower Manhattan Hospital, where he was pronounced dead by an emergency room physician at 7:36 a.m. On August 11, 2019, the Office of the Chief Medical Examiner, City of New York, performed an autopsy on Epstein and determined that the cause of death was hanging and the manner of death was suicide. The OIG conducted this investigation jointly with the Federal Bureau of Investigation (FBI), with the OIG’s investigative focus being the conduct of BOP personnel. Among other things, the FBI investigated the cause of Epstein’s death. The FBI determined that there was no criminality pertaining to how Epstein had died. This report concerns the OIG’s findings regarding MCC New York personnel’s custody, care, and supervision of Epstein during his detention at the facility from his arrest on July 6, 2019, until his death on August 10, 2019. The OIG investigation and review identified numerous and serious failures by MCC New York staff, as well as multiple violations of MCC New York and BOP policies and procedures. Among the most significant was the failure to assign Epstein a new cellmate on August 9, 2019, after Epstein’s cellmate was transferred out of MCC New York that day. Epstein was required to have a cellmate at all times pursuant to a written direction that the MCC New York Psychology Department issued on July 30 after Epstein was removed from suicide watch and psychological observation following a possible attempted suicide by him on July 23. As a result of the failure to assig...
3 that they had conducted all of the required counts of inmates and 30-minute rounds during their shifts within the SHU. As described in greater detail in Chapter 2, inmate counts and 30-minute rounds are two means by which the BOP accounts for inmates and assesses their safety, security, and well-being. BOP and MCC New York policies require that staff members count all inmates in each housing unit within the facility at designated times each day. Additionally, BOP and MCC New York policies require that a staff member observe all SHU inmates at least once during the first 30 minutes of each hour (e.g., 12 a.m. to 12:30 a.m.) and again during the second 30 minutes of the hour (e.g., 12:30 a.m. to 1 a.m.), thus ensuring that inmates are observed at least twice per hour. BOP staff are required to document inmate counts and 30-minute rounds on official BOP forms, which are often referred to as “count slips” and “round sheets.”2 During the OIG’s investigation, the OIG obtained information that the staff assigned to the MCC New York SHU did not conduct any counts of inmates within the SHU from August 9, 2019, at approximately 4 p.m., until Epstein was found hanged in his cell on the morning of August 10, 2019. However, in documentation completed by the SHU staff on duty during that period, staff members falsely certified in the count slips that they had conducted the required counts. Additionally, the OIG investigation revealed that the staff assigned to the MCC New York SHU did not conduct any required 30-minute rounds of inmates after approximately 10:40 p.m. on August 9, 2019. Again, however, SHU staff on duty during that period had falsely certified in the round sheet that the required rounds were conducted. The combination of these and other failures led to Epstein being unmonitored and locked alone in his cell, which the OIG found contained an excessive amount of bed linens, from approximately 10:40 p.m. on August 9 until he was discov...
4 Epstein was housed, from the common area of the SHU between approximately 10:40 p.m. on August 9 and approximately 6:30 a.m. on August 10. Finally, the Medical Examiner who performed the autopsy detailed for the OIG why Epstein’s injuries were more consistent with, and indicative of, a suicide by hanging rather than a homicide by strangulation. The Medical Examiner also cited to the absence of debris under Epstein’s fingernails, marks on his hands, contusions to his knuckles, or bruises on his body that evidenced Epstein had been in a struggle, which would be expected if Epstein’s death had been a homicide by strangulation. As discussed in greater detail in the Conclusions and Recommendations chapter of this report, this is not the first time that the OIG has found significant job performance and management failures on the part of BOP personnel and widespread disregard of BOP policies that are designed to ensure that inmates are safe, secure, and in good health. The OIG has investigated numerous allegations related to the falsification of official BOP documentation concerning inmate counts and rounds and has repeatedly found deficiencies with the BOP’s staffing levels, the custody and care of inmates at risk for suicide, and security camera systems at BOP institutions. The combination of negligence, misconduct, and outright job performance failures documented in this report all contributed to an environment in which arguably one of the most notorious inmates in BOP’s custody was provided with the opportunity to take his own life. The BOP’s failures are troubling not only because the BOP did not adequately safeguard an individual in its custody, but also because they led to questions about the circumstances surrounding Epstein’s death and effectively deprived Epstein’s numerous victims of the opportunity to seek justice through the criminal justice process. The fact that these failures have been recurring ones at the BOP does not excuse...
5 Chapter 2: Background I. Significant Entities and Individuals Jeffrey Epstein was born in 1953 and, prior to his arrest, worked at various jobs in the financial industry and ultimately developed considerable wealth. On July 2, 2019, a federal grand jury of the U.S. District Court for the Southern District of New York returned an indictment that charged Epstein with engaging in sex trafficking and a sex trafficking conspiracy, in violation of 18 U.S.C. §§ 371, 1591(a), (b)(2), and 2. These charges were based on allegations that between 2002 and 2005, Epstein paid girls as young as 14 years old hundreds of dollars in cash each for engaging in sex acts with him at his Florida and New York residences. The indictment further alleged that Epstein also paid each of these minor victims hundreds of dollars in cash to recruit other girls to engage in sex acts with Epstein. On July 6, 2019, Epstein was arrested at Teterboro Airport in New Jersey upon his return to the United States from France and was transported to the Federal Bureau of Prisons’ (BOP) Metropolitan Correctional Center, located at 150 Park Row in New York, New York (MCC New York). Following a detention hearing on July 15, 2019, the court ordered that Epstein be detained pending trial based on the court’s finding that he was a danger to the community and a flight risk. MCC New York is a federal administrative detention facility operated by the BOP that primarily provides pretrial detention services for the U.S. District Courts for the Southern and Eastern Districts of New York. The BOP temporarily closed MCC New York in October 2021 due to substandard conditions that are unrelated to this investigation. When it was operational, MCC New York housed approximately 750 inmates at any given time. Prior to its closure, the majority of MCC New York’s inmate residents were individuals with pending criminal charges (as opposed to individuals who had been convicted of offenses and were ...
6 referred to as a “round sheet”) falsely stating that she and Thomas had conducted such rounds when, in fact, they had not.5 On November 19, 2019, a federal grand jury of the U.S. District Court for the Southern District of New York returned an indictment that charged Noel and Thomas with one count each of conspiracy and multiple counts each of falsification of records, in violation of 18 U.S.C. §§ 371, 1001(a)(3), and 2. The indictment alleged that on August 9, 2019, Noel failed to conduct the mandatory 4 p.m. and 10 p.m. counts of inmates in the MCC New York SHU, and that on August 10, 2019, both she and Thomas failed to conduct the mandatory 12 a.m., 3 a.m., and 5 a.m. counts and mandatory 30-minute rounds within the MCC New York SHU. The indictment further alleged that Noel and Thomas created, certified, and submitted false documentation indicating that the counts and rounds had been done as required to conceal their failure to perform their assigned duties. As a result, it appeared from documentation that prisoners in the SHU, including Epstein, were being regularly monitored when, in fact, no CO had checked on Epstein from approximately 10:40 p.m. on August 9, 2019, until approximately 6:30 a.m. on August 10, 2019, when Epstein was found hanged in his cell. On May 25, 2021, the U.S. Attorney’s Office for the Southern District of New York entered into deferred prosecution agreements with Noel and Thomas. Their respective agreements, which are part of the court record in their cases, included admissions by Noel and Thomas that they falsely certified that they had conducted counts and rounds. The agreements also required each of them to truthfully and completely disclose all information related to their activities and employment with the BOP; be interviewed by the U.S. Attorney’s Office of the Southern District of New York, the FBI, and the OIG; complete 100 hours of community service; refrain from violating the law; and fulfill oth...
7 requested to provide information.6 The BOP employees and contractors we interviewed included employees involved in various aspects of the emergency response, who worked at MCC New York in the days leading up to the response and following the response, as well as other individuals with information pertinent to our investigation. Additionally, the OIG participated in interviews of 15 inmates who had been housed at MCC New York during time periods relevant to our investigation, including three who were housed in the L Tier of the SHU on the day Epstein died.7 Those three L-Tier inmates were housed in cells opposite Epstein’s cell and therefore had a direct line of sight to Epstein’s cell on the night of August 9–10. The OIG also reached out to one of Epstein’s attorneys to discuss the possibility of providing information, but ultimately the attorney declined to be interviewed, citing attorney-client privilege (the attorney-client privilege survives a client’s death) and issues related to ongoing litigation involving Epstein’s estate. The OIG also collected over 127,000 documents, as well as MCC New York video and photographs. Among these were BOP documents, including staff rosters; daily logs and reports; investigative and incident reports; documentation regarding inmate counts and 30-minute rounds; inmate housing assignment documentation; inmate transfer documents; Psychology Department reports and medical records relating to Epstein; Epstein’s institutional phone call records; MCC New York records of Epstein’s visits with his attorneys; electronic communications, including text messages and emails of BOP employees and contractors; MCC New York security camera surveillance video; records from contractors regarding the MCC New York security camera system; service records for MCC New York’s security camera system; MCC New York photographs, including photographs taken of efforts to revive Epstein on the morning of August 10, 2019; BOP polic...
8 in an honest effort to perform official duties.”9 The ethical regulations also mandate that federal employees not use federal property “for other than authorized activities.”10 BOP policy (Program Statement 3420.11, Standards of Employee Conduct) imposes several additional standards of conduct on its employees. At all times, BOP employees must “[c]onduct themselves in a manner that fosters respect for the Bureau of Prisons, the Department of Justice, and the U.S. Government.” Because “[i]nattention to duty in a correctional environment can result in escapes, assaults, and other incidents,” BOP employees “are required to remain fully alert and attentive during duty hours.” BOP policy provides that employees can use government property for authorized purposes only, and further specifies that personal use of government office equipment, such as computers, “will not take place during official working hours.” BOP policy requires that employees “obey the orders of their superiors at all times.” B. False Statements and Lack of Candor Under federal law, “whoever, in any matter within the jurisdiction of the executive…branch of the Government of the United States, knowingly and willfully…makes or uses any false writing or document knowing the same to contain any materially false, fictitious, or fraudulent statement or entry” has violated 18 U.S.C. § 1001(a)(3). The terms “knowingly and willfully” mean that the subject acted with knowledge that the conduct was, in a general sense, prohibited by law. It is not required that the subject was aware of the existence of Section 1001. Under BOP standards of conduct discussed above, employees are required to cooperate fully with official investigations, which includes providing “all pertinent information they may have” and “truthfully responding to questions.” C. Relevant BOP Policies Regarding the Operation of Correctional Facilities 1. Special Housing Units SHUs within BOP facilities are govern...
9 Inmates in the SHU are securely separated from general population inmates and are kept locked in their cell when in their assigned tier within the SHU. As discussed in greater detail in Chapter 4, witnesses told the OIG that SHU inmates are locked in their cells for approximately 23 hours a day. BOP policy provides that, weather and resources permitting, SHU inmates will have the opportunity to exercise outside their quarters 5 hours per calendar week. Under federal regulations and BOP policy, SHU inmates ordinarily have the opportunity to shower at least 3 times a week, typically on different days in 1-hour periods. SHU inmates may also be escorted from their cells by MCC New York staff for visits, including legal visits, court appearances, medical and psychological attention. The MCC New York SHU Post Orders require that all visitors to the SHU be documented in a visitor log, and that any inmate visiting the SHU, such as inmates on work details, be searched visually and with a hand-held metal detector, without exception. The MCC New York SHU Post Orders also require that food carts be searched inside and out before being brought into a SHU cellblock and that all meals be delivered to each inmate’s cell through the food slot in the inmate’s locked cell door. BOP policy provides that inmates housed in the SHU for 30 continuous calendar days are to be examined and interviewed by a mental health staff member to assess the inmate’s adjustment and the threat presented to self or others. BOP policy also requires that all staff assigned to the SHU participate in quarterly training on, among other things, orderly supervision, suicide prevention, and security procedures relating to the unit. When a staff member is assigned to the SHU at the last-minute and has not completed the quarterly training, the staff member must be advised of the general requirements of a SHU post and be permitted to ask questions about the duties. 2. Inmate Account...
10 Center, which maintains the master count of all inmates, and then remain in the unit until the Control Center accepts the count. If a count reported verbally does not match the master count, then the Control Center must notify the Operations Lieutenant and the staff members must recount the inmates. If the second count does not match the master count, then the Operations Lieutenant will order a bed-book count, that is, when inmates are counted using their picture cards, which are on file in the Control Center. A Lieutenant must take at least 1 count in the morning and one in the evening. Correctional staff prepare count slips for each count, which must be prepared in ink, signed by both officers, and retained for 30 days. Count slips may not be altered. BOP policy provides that the “official count will not be cleared until all count slips are received and verified in the Control Center.” b. 30-Minute Rounds The BOP uses additional accountability measures for inmates who are in administrative detention or disciplinary segregation, i.e., for those detained in a SHU. In such cases, a correctional staff member must observe all inmates at least twice an hour, once during the first 30 minutes (e.g., 12 a.m. to 12:30 a.m.) and again during the second 30 minutes (e.g., 12:30 a.m. to 1 a.m.). BOP policy provides that these “rounds are to be conducted on an irregular schedule and no more than 40 minutes apart.” These same requirements for rounds are also described in the Post Orders for the MCC New York’s SHU. c. Documentation Regarding Inmate Status and Confinement BOP policy also provides that each institution must prepare a daily change/transfer sheet, which indicates changes to an inmate’s status, including housing and job assignments and medical convalescence. The MCC New York SHU Post Orders require that correctional staff assigned to the SHU create a SHU file for each inmate housed in that unit and that morning watch officers audi...
11 admission to the institution. The goal of this screening is to determine “the inmate’s security, medical, psychological, and/or other special needs.” The BOP also requires that institutions screen pretrial inmates “returning from court, as events at court may alter the inmate’s separation and/or security needs.” BOP policy further recognizes that there are often “high security, high profile inmates” who may present a significant threat to themselves or others, and that the “need to identify and monitor these inmates regularly is paramount.” b. Suicide Prevention The BOP’s suicide prevention program is governed by federal regulations, 28 C.F.R. §§ 552.40-552.42, which require the BOP to establish a suicide prevention program to identify and manage potentially suicidal inmates. Pursuant to these regulations, when an inmate is identified as being at-risk for committing suicide, BOP staff must place the inmate on suicide watch until the inmate is no longer an imminent risk. BOP policy (Program Statement 5324.08, Suicide Prevention Program) requires that medical staff screen all new inmates, ordinarily within 24 hours, for signs of suicidality. However, at MCCs, among other facilities with high rates of admissions and short lengths of stays, “comprehensive psychological intake conducted by Psychology Services ordinarily will be performed only on inmates who are suspected of being suicidal or appear psychologically unstable.” Inmates in the SHU are monitored more closely, and inmates exhibiting signs of potential suicide risk are referred to the shift Lieutenant. BOP policy recognizes that inmates who are placed in the SHU due to a request for protective custody are at greater risk of committing suicide and should therefore be screened for suicidal ideation within 72 hours of arriving in the SHU. BOP policy explicitly states that “staff must never take lightly any inmate suicide threats.” Any staff member who has reason to believe tha...
12 4. Suicide Response Recognizing that failure to appropriately respond to an emergency can jeopardize the safety of staff and inmates and the security of the institution, the BOP’s Standards of Employee Conduct require that “employees respond immediately, effectively, and appropriately during all emergency situations.” The MCC New York General Housing Unit Post Orders outline the required response to a suspected inmate suicide. These orders require that MCC New York staff notify the Operations Lieutenant and Control Center of the situation. The orders further provide that, once there is adequate staff present, immediate action must be taken to open the inmate’s airway and initiate cardiopulmonary resuscitation, even if MCC New York staff believe that the inmate “has been dead for a period of time.” MCC New York staff are to continue cardiopulmonary resuscitation until they are relieved by medical staff or another rescuer. The BOP policy governing crime scenes and the collection of evidence provides that the need to immediately attend to an apparent suicide victim, undertake lifesaving measures, and ensure inmate and staff safety take precedence over efforts to preserve a crime scene.13 5. Inmate Discipline Federal regulations, 28 C.F.R. §§ 541.1-541.8, and BOP policy (Program Statement 5270.09, Inmate Discipline Program) establish an inmate discipline program, which is designed to ensure the safety, security, and orderly operation of correctional facilities, as well as the protection of the public. The inmate discipline program applies to all inmates in BOP custody, including inmates with pending criminal charges. One of the guiding principles of this program is that BOP staff are to take disciplinary action when and to such a degree as necessary to regulate the behavior of inmates to promote a safe and orderly institution. “Tattooing or self-mutilation” is among the prohibited acts sanctioned through the inmate discipline program....
13 choose a staff representative, make a statement, and call witnesses. The inmate is also allowed to appeal the outcome through the BOP’s administrative remedy program. 6. Conditions of Confinement a. Telephone Calls The federal regulations, 28 C.F.R. §§ 540.100-540.106, that govern telephone calls for inmates require that the Warden of each BOP institution establish procedures to monitor inmate telephone conversations, which is “done to preserve the security and orderly management of the institution and to protect the public.” For safety and security reasons, BOP policy (Program Statement P5264.08, Inmate Telephone Regulations) requires that all inmate telephone calls be made through the Inmate Telephone System. BOP policy recognizes that “on rare occasion, during times of crisis,” inmates may be permitted to make a telephone call outside of the Inmate Telephone System. In such circumstances, the telephone “must be placed in a secure area (e.g., a locked office),” and “must be set to record telephone calls.” Additionally, the staff member coordinating the call must notify the BOP’s Special Investigative Services via email, providing the inmate’s name and register number, the date and time of the call, the number and name of the individual called, and the reason for the call. The Special Investigative Services must enter this information into the telephone recording system within 7 days. b. Personal Effects, Medication, and Linens Federal regulations governing BOP SHUs provide that inmates in administrative detention status ordinarily may have a reasonable amount of personal property.15 Under BOP policy regarding SHUs, the personal property of SHU inmates “may be limited or withheld for reasons of security, fire safety, or housekeeping.”16 The BOP Chief Pharmacist issues medication each workday for inmates in the SHU. Restricted medications are administered to inmates during daily SHU rounds. Each institution determines “the me...
14 Chapter 3: Timeline of Key Events Except as otherwise noted, the following information is derived from the Federal Bureau of Prisons (BOP) records and the Office of the Inspector General’s interviews. September 21–24, 2018 The BOP awards contracts to two companies (Company 1 and 2) to upgrade the security camera system at Metropolitan Correctional Center in New York, New York (MCC New York). At the time, images from the MCC New York’s analog video cameras are recorded to a Digital Video Recorder (DVR) system, which is divided into two DVR systems. Cameras assigned to the DVR 1 system record only to the DVR 1 hard drives, and cameras assigned to DVR 2 system record only to the DVR 2 hard drives. March 17, 2019 In connection with MCC New York’s upgrade of its security camera system, the BOP’s Northeast Regional Office begins arranging for technicians from other BOP institutions to perform temporary duty (TDY) assignments to MCC New York to perform necessary mechanical, electrical, plumbing, and wiring work. However, during the course of the TDY rotations, work is not consistently conducted on the camera upgrade because TDY personnel are sometimes used to cover shortages at MCC New York’s custody posts. July 2, 2019 According to court records, a federal grand jury of the U.S. District Court for the Southern District of New York returns an indictment charging Epstein with sex trafficking and conspiracy to commit sex trafficking. July 6, 2019 Epstein is arrested at an airport in New Jersey and is transported for detention pending his initial court appearance to the MCC New York as a pretrial detainee. Epstein is placed in the general inmate population and medically screened. July 7, 2019 An MCC New York Facilities Assistant asks the Psychology Department to evaluate Epstein because he appears “distraught, sad, and a little confused.” Epstein is assigned to the MCC New York’s Special Housing Unit (SHU) because of significant...
15 July 8, 2019 According to court records, Epstein is arraigned in federal court and enters a plea of not guilty to all charges. The court sets a detention hearing for July 15, 2019. MCC New York staff conducts a routine intake screening of Epstein, the records of which indicate that Epstein denies a history of any mental health problems. After the Chief Psychologist consults with the National Suicide Prevention Coordinator from BOP’s Central Office, the Psychology Department conducts a further evaluation of Epstein after his return from court. Records show that Epstein denies any suicidal thoughts but was placed on psychological observation due to the presence of risk factors (high-profile case, nature of the charges, pre-trial status, and ongoing proceedings). July 9, 2019 The Psychology Department administers a formal, in-person suicide risk assessment for Epstein. The Psychology Department continues psychological observation for another day pending a suitable housing placement. July 10, 2019 The Psychology Department removes Epstein from psychological observation and returns him to the SHU with a recommendation that he have a cellmate. Epstein is housed with another inmate (Inmate 1). July 11, 2019 An MCC New York psychologist meets with Epstein briefly and recommends follow-up visit to occur the next week. July 15, 2019 According to court records, Epstein appears in court for his detention hearing. July 16, 2019 At Epstein’s request, an MCC New York psychologist meets with him during a legal visit. July 18, 2019 According to court records, Epstein appears in court for a ruling on the issue of detention. The court orders that Epstein be detained pending trial because he presents a danger to the community and he is a flight risk. The Psychology Department conducts 30-day psychology reviews for the entire SHU population. Epstein is not in the SHU at the time and therefore his review is not conducted.
16 July 22, 2019 According to court records, Epstein files an appeal of the court’s order denying Epstein pretrial release. July 23, 2019 At approximately 1:27 a.m., SHU staff hears noises coming from Epstein’s cell. Epstein’s cellmate (Inmate 1) says that Epstein has attempted to hang himself. SHU staff observes Epstein lying on the floor with a piece of orange cloth around his neck. Epstein initially tells MCC New York staff that his cellmate tried to kill him. Epstein’s cellmate (Inmate 1) tells MCC New York staff that while he was asleep, he felt something hit his legs and when he turned on the light, he saw Epstein with a string around his neck and called the guards.18 Epstein is transferred out of the SHU and placed on suicide watch in a cell near the Psychology Department and Health Services Unit. Later that morning, Health Services Unit personnel conduct a medical assessment and observe that Epstein has a red mark two-thirds of the way around the front and sides of his neck. The BOP assesses Epstein for risk of suicide and determines that he should remain on suicide watch. July 24, 2019 At approximately 8:45 a.m., Epstein is removed from suicide watch but remains under psychological observation in the same cell near the Psychology Department and Health Services Unit. Medical staff examine Epstein at 1:08 p.m. and Psychological Services staff complete a Post Suicide Watch Report. In contrast to his prior statement that his cellmate tried to kill him, Epstein says he does not remember how he sustained the injuries to his neck. July 25–29, 2019 Epstein is seen by the Psychology Department daily and on each date adamantly denies suicidality or having any memory of what occurred on July 23, 2019. July 29, 2019 Psychology Department staff determine that Epstein can be released from psychological observation and transferred back to the SHU.19 18 When interviewed by the OIG, another inmate housed in the same SHU tier (...
17 Disk failures occur in DVR 2 of MCC New York’s security camera system, which results in the system being unable to record, although the cameras continue to work and broadcast live video feed. MCC New York personnel do not learn of the DVR 2 recording failure until August 8, 2 days before Epstein’s death. Roughly half of MCC New York’s security cameras, including those located in the SHU, are assigned to record to the DVR 2 system. July 30, 2019 Epstein is transferred back to the SHU.20 An MCC New York Staff Psychologist from the Psychology Department sends an email to over 70 BOP staff members stating that Epstein “needs to be housed with an appropriate cellmate.” Epstein and his new cellmate (Inmate 3) are placed in a cell within the SHU that can accommodate the electrical needs of Epstein’s medical device. MCC New York conducts disciplinary proceedings against Epstein for alleged self-mutilation and ultimately concludes that there is insufficient evidence to find that Epstein engaged in a prohibited act.21 When Epstein is psychologically evaluated in connection with the disciplinary proceedings, he says he does not remember how he sustained the marks around his neck. MCC New York personnel attempt to obtain an estimate from Company 1 to run the wiring and conduit for the new camera system, which would eliminate the need for BOP technicians to perform the work. July 31, 2019 According to court records, Epstein appears in court for a status conference, at which time the court sets deadlines for motions and responses. Upon his return to MCC New York, the U.S. Marshals Service provide paperwork to BOP that indicates Epstein had “suicidal tendencies.” database that contains information relating to the care, classification, subsistence, protection, discipline, and programs of federal inmates, was not updated to reflect this change because it indicated that Epstein was transferred back to the SHU on July 29, 2019. 20 The OI...
18 The Psychology Department conducts a clinical visit with Epstein, who denies any suicidal ideation. August 1, 2019 MCC New York Receiving and Discharge staff notify the Psychology Department of the notation of “suicidal tendencies” on U.S. Marshals Service paperwork relating to Epstein. The Psychology Department conducts a suicide risk assessment of Epstein, who denies that he is suicidal, and determines that suicide watch is not warranted. Psychological staff recommend a follow-up in 1 week. August 2, 2019 MCC New York Special Investigative Services complete its investigation into the incident on July 23, 2019, and finds that there is insufficient evidence to determine that Epstein harmed himself or that he was harmed by his cellmate. August 8, 2019 Epstein is seen by the Psychology Department and denies suicidal ideation, intention, or plan. Epstein meets with his attorneys and, unbeknownst to MCC New York personnel, changes his Last Will and Testament during the meeting. MCC New York staff receive notice that Epstein’s cellmate will be transferred out of the institution the following day, August 9. MCC New York staff discover the disk failures that occurred in the DVR 2 system on July 29 and that resulted in approximately one half of the institution’s security cameras not recording, although the cameras continued to broadcast a live video feed. MCC New York staff do not perform the work necessary to restore recording functionality of the DVR 2 system or address long-standing performance failures with the institution’s camera system. August 9, 2019 At approximately 8:30 a.m., Epstein’s cellmate (Inmate 3) is transferred out of MCC New York. Two MCC New York SHU staff members said they notified supervisory staff of Epstein’s cellmate’s transfer and Epstein’s need for a new cellmate. Other witnesses did not corroborate these statements. Epstein is not assigned a new cellmate as required by the Psychology Department. So...
19 attorneys ask MCC New York staff members if Epstein could be moved to a different housing unit or housed without a cellmate. MCC New York staff obtain the replacement hard drives to repair the institution’s security camera system but do not complete the repairs necessary to restore recording functionality and address long-standing performance failures with the institution’s DVR 2 system. The U.S. Court of Appeals for the Second Circuit unseals approximately 2,000 pages of documents in civil litigation involving Ghislaine Maxwell, who is later convicted in December 2021 of conspiring with Epstein to sexually abuse minors over the course of a decade. Some of these documents contain information that may relate to the criminal charges pending against Epstein. There is extensive media coverage of information in the unsealed documents. At approximately 6:45 p.m., Epstein leaves the attorney conference room. At approximately 7 p.m., contrary to BOP policy but with the permission of a Unit Manager, Epstein is permitted to place an unmonitored telephone call to a number with a New York City area code, purportedly to speak with his mother. In actuality, Epstein speaks with someone with whom he allegedly has a personal relationship. After the call, Epstein is returned to his cell, where he remains without a cellmate. MCC New York SHU staff members do not conduct the 4 p.m. or 10 p.m. inmate counts. After approximately 10:40 p.m., SHU staff members do not conduct the required 30-minute rounds. August 10, 2019 MCC New York SHU staff members do not conduct the 12 a.m., 3 a.m., or 5 a.m. inmate counts or any of the 30-minute rounds from 12 a.m. until approximately 6:30 a.m. At approximately 6:30 a.m., SHU staff begin to deliver breakfast to inmates in the SHU through the food slots in the locked cell doors. When SHU staff attempt to deliver breakfast to Epstein, SHU staff unlock the door to the tier in which Epstein’s cell was located an...
20 buttocks approximately 1 inch to 1 inch and a half off the floor and his legs extended straight out on the floor in front of him. SHU staff immediately activate a body alarm, which notified all MCC New York staff of a medical emergency and prompted MCC New York staff in the Control Center to call for 911 emergency services. SHU staff then rip the orange cloth away from the bunkbed, which causes Epstein’s buttocks to drop to the ground. SHU staff lay Epstein on the ground and immediately initiate cardiopulmonary resuscitation (CPR). At approximately 6:33 a.m., BOP medical staff respond to the SHU, continue CPR, apply the automated external defibrillator, and move Epstein to MCC New York’s Health Services Unit. Minutes after arriving in the Health Services Unit, an ambulance arrives and paramedics continue CPR, intubate Epstein, and administer medications and fluids. At approximately 7:10 a.m., the ambulance takes Epstein to New York Presbyterian Lower Manhattan Hospital, where he is pronounced dead at 7:36 a.m. by the emergency room physician. MCC New York staff unsuccessfully attempts to recover video from the DVR 2 system of the SHU and the BOP begins repairing the DVR 2 system. The FBI seizes all hard drives contained in the DVR 2 system as evidence. August 11, 2019 The Office of the Chief Medical Examiner, City of New York, conducts an autopsy of Epstein. August 14–15, 2019 The FBI returns to MCC New York and seizes additional components of the DVR 2 system and the entire DVR 1 system. The FBI’s Digital Forensics Analysis Unit in Quantico, Virginia, begins to conduct a forensic analysis of MCC New York’s DVR systems and determines that there were catastrophic disk failures in the DVR 2 system disk array and no recordings were available on the DVR 2 system after July 29, 2019. August 16, 2019 The Office of the Chief Medical Examiner, City of New York, releases its findings publicly that the cause of Epstein’s death was...
21 Chapter 4: Custody and Care of Epstein Prior to His Death I. Epstein’s Arrest and Detention on July 6 On July 2, 2019, a grand jury of the U.S. District Court for the Southern District of New York returned a two- count indictment that charged Epstein with committing sex trafficking and a sex trafficking conspiracy, in violation of 18 U.S.C. §§ 371, 1591(a), (b)(2), and 2, based on allegations that he sexually exploited and abused dozens of minor girls, some as young as 14 years old, at his homes in New York and Florida. The indictment alleged that from at least 2002 through 2005, Epstein enticed and recruited girls, many of whom he knew were underage, to visit his homes and perform sex acts in exchange for paying each girl hundreds of dollars in cash. The indictment further alleged that Epstein, working with employees and associates, created a vast network of underage victims to sexually exploit in New York and Florida by paying some victims hundreds of dollars in cash each to recruit other minor girls to be similarly abused by Epstein. In addition to the two criminal charges, the indictment also contained forfeiture allegations, which sought to forfeit to the United States any property that was either used to commit or was a proceed of the charged sex trafficking offense, including Epstein’s New York residence. On Saturday, July 6, 2019, Epstein was arrested at Teterboro Airport in New Jersey upon his return to the United States from France. He was transported to the Metropolitan Correctional Center located in New York, New York (MCC New York), where he was initially placed in the general inmate population. MCC New York is a federal administrative detention facility operated by the Federal Bureau of Prisons (BOP). The BOP temporarily closed MCC New York in October 2021 due to substandard conditions that are unrelated to this investigation. When it was operational, MCC New York housed primarily pretrial detainees who had not yet b...
22 obligations as a registered sex offender. The court found that the United States had also shown by a preponderance of the evidence that Epstein was a flight risk based on the severity of the criminal charges and severity of the potential punishment; the strength of the evidence against Epstein; and Epstein’s criminal history, sex offender registration, vast wealth and substantial liquid assets, multiple residences, a foreign residence, limited family ties in the United States, private plane(s), extensive overseas travel, and possession of a foreign passport bearing Epstein’s photograph but not his name. Finally, the court found that Epstein’s pretrial release proposal was inadequate because, among other things, it did not contain sworn, accurate, or comprehensive financial statements; it required excessive court involvement in routine aspects of the proposed home confinement; the proposed consent to extradition was unenforceable; and the proposed appointment of a trustee to monitor Epstein’s compliance with release conditions was unacceptably vague and problematic due to the potential conflict of interest presented by monitoring the conduct of a person who paid the trustee’s salary, and allegations that Epstein engaged in unlawful acts with his employees during the sex trafficking conspiracy. Epstein appealed the court’s order on July 22, 2019. This appeal remained pending at the time of Epstein’s death. II. MCC New York’s Special Housing Unit Epstein was initially assigned to MCC New York’s general inmate population, but on July 7, 2019, at approximately 7:20 p.m., he was moved to the SHU pending reclassification due to the significant increase in media coverage and awareness of his notoriety among other MCC New York inmate residents. The SHU is a housing unit within MCC New York where inmates are securely separated from the general inmate population and kept locked in their cells for approximately 23 hours a day, to ensure their ow...
23 meet with their clients because Epstein and his attorneys were occupying the attorney conference room, even at times when Epstein had to leave the conference room for a medical visit. At MCC New York, the SHU was located on the south side of the institution’s ninth floor and was often referred to as “9 South.” Primary access to the SHU was controlled by a locked door (Main Exterior Entry Door). That door was opened remotely by a staff member in MCC New York’s centralized Control Center. Access into the SHU was further controlled by a second locked door (Main Interior Entry Door), to which a limited number of Correctional Officers (CO) had keys while on duty. Secondary access to the SHU was controlled by a locked door. That door was opened remotely by a staff member in the centralized Control Center. Entry into the SHU from the secondary access point was further controlled by three additional locked doors, to which a limited number of the COs had keys while on duty. The secondary access doors were used only by staff when facilitating visits between the SHU inmates and their outside visitors. Within the SHU, inmates were assigned to six separate tiers or groups of cells, three of which were accessible via stairs leading up from the common area on the ninth floor (Upper Tiers—G, J, and L Tiers) and three of which were accessible via stairs leading down from the common area on the ninth floor (Lower Tiers—H, K, and M Tiers). The entrance to each tier could be accessed only via a single locked door at the top or bottom of the staircase leading to the individual tier. A limited number of keys to open the locked tier doors were available only to a limited number of COs while on duty. Each tier had eight cells, each of which could house either one or two inmates. Each individual cell, which was made of cement and metal, could be accessed only through a single locked door, to which only a limited number of COs had keys while on duty. Th...
24 Figure 4.1 Primary SHU Entrance (Ninth Floor) Note: The photograph on the right has been modified for security reasons. Source: DOJ OIG photographs and DOJ OIG schematic drawing depicting the MCC New York SHU
25 Figure 4.2 Secondary SHU Entrance (Ninth Floor) Note: The photograph on the right has been modified for security reasons. Source: DOJ OIG photographs and DOJ OIG schematic drawing depicting the MCC New York SHU Main Entry Door (not pictured)
26 Figure 4.3 Tiered Structure of SHU (2-Dimensional) Source: DOJ OIG schematic drawings depicting the MCC New York SHU Upper Tiers Lower Tiers
27 Figure 4.4 Tiered Structure of SHU (3-Dimensional) Source: DOJ OIG schematic drawing depicting the MCC New York SHU
28 Figure 4.5 Stairways Leading to SHU Upper and Lower Tiers Note: The photograph on the right has been modified for privacy reasons. Source: DOJ OIG photographs and DOJ OIG schematic drawing depicting the MCC New York SHU III. Epstein’s Initial Cell and Cellmate Assignment from July 7 to July 23 According to the Warden, MCC New York typically housed inmates in the SHU with a cellmate. Upon Epstein’s initial transfer to the SHU on July 7, 2019, he was assigned a cell in the M Tier of the SHU with Inmate 1. The Warden explained that Epstein was a high-profile inmate and that he initially selected Inmate 1 to be Epstein’s cellmate because Inmate 1 was another high-profile inmate, and the Warden believed Inmate 1 to be the least likely SHU inmate to harm Epstein.23 Epstein and Inmate 1 were housed together in cell Z05-124. 23 In 2008, Epstein pleaded guilty in a Florida state court to a felony charge of procurement of minors to engage in prostitution in violation of Florida Statute § 796.03. As a result of this conviction, Epstein was required to register as a sex offender.
29 IV. Events of July 23 and the Placement of Epstein on Suicide Watch and Psychological Observation from July 23 to July 30 According to BOP documents, at approximately 1:27 a.m. on July 23, 2019, Senior Officer Specialists 1 and 2 heard noise coming from the M Tier in the SHU, the tier where Epstein was housed. Senior Officer Specialist 2 documented in a BOP report that upon checking cell Z05-124, he saw Epstein laying down near his bunk with “a piece of handmade orange cloth” around his neck, and Senior Officer Specialist 1 wrote in a BOP report that Epstein’s cellmate (Inmate 1) said Epstein had attempted to hang himself. In his interview with the OIG, Senior Officer Specialist 1 said that Inmate 1, who appeared shaken up, told him that he had been asleep on the floor of the cell and was awoken when he felt Epstein land on him. Senior Officer Specialist 2 reported that after he had been alerted by the noise, he grabbed the door keys, called the Control Center for assistance, and then he and Senior Officer Specialist 1 entered the cell, where they secured and removed Epstein’s cellmate. Senior Officer Specialist 1 reported that he then reentered the cell, placed Epstein on his side, and removed “an orange homemade rope” from his neck. In his interview with the OIG, Senior Officer Specialist 1 said Epstein had a sheet around his neck, which was attached to the bunkbed ladder in the cell. Senior Officer Specialist 1 said that Epstein was sitting on the floor of the cell with his back against the bunkbed ladder. Senior Officer Specialist 1’s report said that Epstein was breathing, but unresponsive, so he began chest compressions, at which time the Morning Watch Operations Lieutenant and other staff arrived. Senior Officer Specialist 1 confirmed in his OIG interview that they started cardiopulmonary resuscitation but stopped when they realized that Epstein was already breathing. The Morning Watch Operations Lieutenant documented in a...
30 The Morning Watch Operations Lieutenant documented in a BOP report that when she returned to the Health Services Unit, Senior Officer Specialist 4 informed her that Epstein had said that his cellmate had tried to kill Epstein and had been harassing him. The Morning Watch Operations Lieutenant then spoke with the cellmate (Inmate 1), who said he was wearing headphones and was asleep when he felt something hit his legs. Inmate 1 said he called out to Epstein and when Epstein did not answer, he got up, turned on the light, and saw Epstein sitting on the floor, leaning to the side with a string around his neck. Inmate 1 told the Morning Watch Operations Lieutenant that he then called the guards. Inmate 1 provided a similar statement to BOP officials at approximately 2:50 p.m. on July 23, 2019. The Morning Watch Operations Lieutenant’s report notes that she also spoke with Epstein, who told her that he had returned to his cell after an attorney visit at approximately 8 p.m. the previous day, at which time his cellmate was reading the Daily News newspaper. Epstein’s said his cellmate turned to a page of the newspaper that had Epstein’s picture and reported that Epstein was worth $77 million. Epstein told the Morning Watch Operations Lieutenant that he looked at his picture, balled it up, and threw it in the garbage. Epstein further stated that he woke up at approximately 1 a.m. to get a drink of water, returned to his bunk, and the next thing he remembered was that he was snoring and MCC New York staff were inside his cell. When asked about the allegations against his cellmate, Epstein said he had been told that if his cellmate hurt him, MCC New York staff would not care. Inmate 2, who was housed in the same SHU tier as Epstein on July 23, told the FBI about an incident that occurred in the SHU around 1:20 a.m. to 1:30 a.m. on an unspecified date. Inmate 2 said he was reading a book when he heard an inmate scream and bang on the cell do...
31 believed that his cellmate had something to do with it. BOP’s Special Investigative Services (SIS) opened an investigation into this incident but was unable to determine whether Epstein harmed himself or had been assaulted. On July 24, 2019, at approximately 8:45 a.m., Epstein was removed from suicide watch. However, Epstein remained in the same cell that he was placed in the previous day and was under psychological observation until July 30, 2019.24 The MCC New York Chief Psychologist told the OIG that an inmate is placed on suicide watch when the inmate is believed to be imminently suicidal. During suicide watch, the inmate is under constant observation by staff; the cell lights are on 24 hours a day; and the inmate is given a special mattress, blanket, and smock to wear. The Chief Psychologist explained that although psychological observation is a lower classification, at MCC New York the psychological observations were the same as suicide watch except that inmates were allowed to have their clothing and some materials, such as books, as determined by Psychology Department. At MCC New York, psychological observation was used to see how an inmate was doing before releasing the inmate to a housing unit. The Chief Psychologist told the OIG that the Psychology Department independently makes the decision who goes on and off suicide watch. The Chief Psychologist also stated that the Psychology Department makes recommendations to the institution’s management about where inmates are housed when they come off of suicide watch. According to her, the Psychology Department always recommends that inmates coming off of suicide watch be housed with other inmates; however, she said the recommendations cannot always be carried out due to other security factors. When that occurs, the Psychology Department recommends conducting increased rounds and keeping an eye on those inmates. The Chief Psychologist further told the OIG that, based on a conv...
32 Senior Officer Specialist 1 told the OIG that after Epstein came off of suicide watch, Epstein asked if he could be paired up with Inmate 1 again. Senior Officer Specialist 1 told Epstein that his request was something he would need to raise with the Operations Lieutenant. Senior Officer Specialist 1 told the OIG that Epstein replied, “Yeah, but I don’t understand, you know, we were bunkies, everything was cool.” The Chief Psychologist also told the OIG that Epstein mentioned to her that he wanted Inmate 1 to continue to be his cellmate. V. The Psychology Department’s Post-July 23 Determination that Epstein Needed to Have an Appropriate Cellmate Following the events of July 23, the MCC New York Psychology Department determined that Epstein needed to be housed with an appropriate cellmate. To ensure Epstein’s cellmate requirement was disseminated to MCC New York staff, on July 30, 2019, at 12:30 p.m., the Staff Psychologist sent an email to over 70 MCC New York staff members which read, “Inmate Epstein #76318-054 is being taken off Psych Observation and needs to be housed with an appropriate cellmate.” A review of the email recipients showed that the email was sent to, among others, the Warden, Associate Warden 2, the Captain, the SHU Lieutenant, the SIS Lieutenant, the Day Watch Operations Lieutenant, the Evening Watch Operations Lieutenant, the Morning Watch Operations Lieutenant, the Day Watch Activities Lieutenant, and CO 1. The Staff Psychologist also completed a “Post-Watch Report,” which stated that the “SHU L[ieutenant] informed inmate Epstein needs to be housed with an appropriate cellmate.” The Warden told the OIG that the Chief Psychologist had advised him that Epstein was not suicidal and was ready to return to the SHU. According to the Warden, when he spoke with the Chief Psychologist regarding Epstein, she told him to assign Epstein a cellmate. He added that MCC New York would typically house an inmate who was previ...
33 common practice in the BOP for prisoners coming off of suicide watch to be assigned a cellmate. The SHU Lieutenant confirmed that a BOP psychologist told him that Epstein had to be housed with a cellmate when Epstein returned to the SHU and said that he passed the directive down to the SHU staff. Additionally, the Day Watch SHU Officer in Charge on August 9, 2019, said he and all other SHU staff were aware of Epstein’s cellmate requirement. MCC New York Psychology Department personnel told the OIG that MCC New York staff members knew of Epstein’s cellmate requirement because it was discussed during staff meetings, department head meetings, SHU meetings, morning meetings, and during required staff training. Forensic Psychologist 1 told the OIG that on August 9, 2019, she was present during a meeting in which one of Epstein’s attorneys opposed Epstein having a cellmate. Forensic Psychologist 1 said she explained to the attorney that Epstein needed to have a cellmate because he was housed in the SHU and he was a sex offender. VI. Selection of Epstein’s Cellmate After Psychological Observation The Captain told the OIG that he compiled a list of possible cellmates for Epstein, vetted those inmates, and provided the list of names to the MCC New York Warden. The Warden told the OIG that he identified two potential cellmates and tentatively decided on Inmate 3. The Warden said he passed this information on to the BOP Director’s Chief of Staff and later received word that he should assign Inmate 3 to be Epstein’s cellmate. The Warden told the OIG that no inmates were pre-vetted to replace Inmate 3 if he left MCC New York. The Warden and the Captain told the OIG that if Inmate 3 had been removed as Epstein’s cellmate, they would have had to review a new list of potential cellmate candidates to ensure that Epstein was housed with an appropriate inmate. According to the Warden and the Captain, if Inmate 3 was no longer detained at MCC New Y...
34 medical record note reflected that, on this same date, Epstein was provided with his personally-owned medical device. BOP witnesses told the OIG that on that same date, Epstein and Inmate 3 were moved to cell Z06-220 in the L Tier of the SHU to accommodate the electrical needs of Epstein’s medical device. Of all the cells in the SHU, cell Z06-220 was the closest cell with a direct line of sight to the SHU Officers’ Station in the common area of the SHU, which was approximately 15 feet away. Inmate 3 told the OIG that when he and Epstein were first assigned as cellmates in cell Z06-220 in the L Tier, the Day Watch Operations Lieutenant told Inmate 3 that he had a “cool bunkie” for him, an “old guy” who would not bother Inmate 3. Inmate 3 said he told the Day Watch Operations Lieutenant that he slept on the bottom bunk, and the Day Watch Operations Lieutenant said that would not be a problem because his new cellmate slept on the floor. Inmate 3 said he was surprised by this response because he understood that sleeping on the floor was not allowed and he had previously been disciplined for doing so. When Epstein arrived in the cell, Inmate 3 recognized him and said he (Inmate 3) told the Day Watch Operations Lieutenant that the Day Watch Operations Lieutenant had “jammed up” Inmate 3. Inmate 3 said he knew Epstein had tried to hang himself and had just come from suicide watch. According to Inmate 3, the Day Watch Operations Lieutenant told Inmate 3 not to worry, that Epstein was okay, and that Inmate 3 should keep an eye on him. Inmate 3 asked the Day Watch Operations Lieutenant if he was supposed to serve as a suicide prevention advocate, that is, an inmate who is assigned to the suicide watch area. Inmate 3 said the Day Watch Operations Lieutenant laughed and brushed off Inmate 3’s comment. According to Inmate 3, COs brought two mattresses to the cell for Epstein and placed them on the floor. Epstein put the mattresses on the right...
35 Figure 4.6 SHU L Tier Sources: DOJ OIG schematic drawing depicting the MCC New York SHU; and photograph taken by the Office of the Chief Medical Examiner, City of New York (OCME)
36 Figure 4.7 Exterior Views of Epstein’s Cell Note: Both photographs have been modified for security reasons and the left photograph has been modified for privacy reasons. Sources: DOJ OIG schematic drawing depicting the MCC New York SHU; OCME photographs
37 Figure 4.8 The Door to the Cell Occupied by Epstein and Inmate 3 from July 30 to August 9 Note: The photograph has been modified for privacy reasons. Source: OCME
38 Figure 4.9 View of Epstein’s Empty Cell from Cell Door Window Source: DOJ OIG photograph and DOJ OIG schematic drawing depicting the MCC New York SHU
39 Figure 4.10 Interior View of Epstein’s Empty Cell from Just Inside the Cell Door Source: DOJ OIG photograph and DOJ OIG schematic drawing depicting the MCC New York SHU
40 Figure 4.11 View of Epstein’s Cell Door from the SHU Officers’ Station Note: The photograph has been modified for security and privacy reasons. Source: DOJ OIG photograph and DOJ OIG schematic drawing depicting the MCC New York SHU
41 Figure 4.12 View of the SHU Officers’ Station from Epstein’s cell Note: The photograph has been modified for security reasons. Source: DOJ OIG photograph and DOJ OIG schematic drawing depicting the MCC New York SHU VIII. Psychological Evaluations of Epstein from July 6 to August 9 During Epstein’s detention at MCC New York, a variety of medical professionals, including a Medical Doctor, a Clinical Nurse, and Physician Assistant 1, who is a Mid-Level Practitioner, conducted multiple medical appointments with Epstein, and Epstein was prescribed a variety of medications for various ailments and health needs. Epstein was also given an eye and dental exam, as well as a blood panel screening. This section details Epstein’s psychological evaluations while he was in MCC New York custody prior to his death. On Saturday, July 6, 2019, at 9:38 p.m., upon Epstein’s intake into MCC New York, he was medically screened by Physician Assistant 2. The screening included taking vital signs and asking various medical history questions, including questions related to Epstein’s mental health. Among other things, Physician Assistant 2 annotated that Epstein did not have current suicidal ideation and had denied having a history of suicide attempts. Physician Assistant 2 instructed Epstein how he could obtain medical, dental, and mental health care. At 2:58 a.m. on Sunday, July 7, 2019, a Facilities Assistant emailed the Psychology Department asking that someone evaluate Epstein because he appeared “distraught, sad, and a little confused.” On July 8, 2019, Forensic Psychologist 1 of the Psychology Department conducted an Intake Screening of Epstein that included a self-report, staff observation, and a review of information in SENTRY. Forensic
42 Psychologist 1 noted that during Physician Assistant 1’s initial intake evaluation, on the intake questionnaire, Epstein denied having a history of mental health treatment and any history of mental health symptoms. Additionally, Forensic Psychologist 1 noted no suicidal ideations, attempts, or self-harm; no history of substance abuse or treatment; and no sexual offense convictions. During the evaluation, Epstein stated he had been previously incarcerated for 3 months for “prostitution,” and that he was currently charged with sex trafficking. Epstein denied recent or present morbid thoughts and denied passive or active suicidal ideation. It was noted in BOP records that Epstein’s verbalizations were future-oriented and did not have indications of helpless or hopeless thinking. According to Forensic Psychologist 1, Epstein did not meet the criteria for any psychological diagnosis and was designated as Mental Health Care Code 1. This is indicative of an inmate who does not show any significant level of functional impairment associated with a mental illness and does not demonstrate a need for regular mental health intervention. Epstein was educated on emergency procedures for contacting the Psychology Department staff, and Epstein agreed to contact staff if he needed Psychology Department services in the future. The MCC New York Chief Psychologist told the OIG that based on the Psychological Services Intake Questionnaire, inmates have four different Care Code ratings.27 Code 1 means there are no concerns about the inmate’s mental health status; they have no needs and will not be followed up with unless requested by staff or the inmates. Code 2 means there is some history of mental health issues, but the inmate has them under control and the Psychology Department will follow up monthly. Code 3 is more severe, requiring weekly visits by the Psychology Department to ensure the inmate is stable and if unstable would be moved to observatio...
43 companion program at an institution to utilize inmate observers, who are selected, trained, and supervised by the institution’s Suicide Prevention Program Coordinator. On July 9, 2019, the Chief Psychologist conducted a suicide assessment of Epstein. She reviewed Epstein’s medical record and interviewed him, which revealed that he possessed some risk factors for suicidality. Epstein denied having any past or present suicidal ideation, intention, or plan, and also denied having any history of mental health treatment or any current mental health symptoms. The Chief Psychologist’s assessment was that Epstein had “protective” factors present that could decrease his risk of suicide. The Chief Psychologist assessed factors that included his willingness to engage in treatment, view of death as negative, future orientation, and the fact that he adamantly denied any suicidal ideation, intention, or plan. The Chief Psychologist’s assessment was that Epstein had numerous protective factors that outweighed his risk factors for suicidality and that he had a positive outlook regarding his legal case. Epstein remained on psychological observation pending a suitable cell assignment, and the Chief Psychologist noted that a suicide watch was not warranted at the time of her report. On July 10, 2019, the Chief Psychologist met with Epstein for a psychological observation and noted that, according to the psychological observation logbook, Epstein had been eating his meals, sleeping, and interacting with other inmates. During this meeting with the Chief Psychologist, Epstein voiced concerns over being housed in the SHU. Epstein asked the Chief Psychologist to be “single-celled” if he were to be housed in the SHU and had also requested a shower, his property, pen, and paper. The Chief Psychologist stated Epstein had been provided a shower on this date. She provided Epstein with coping skills strategies, to which he was receptive. Epstein continued to...
44 scheduled to be seen again the following week. The Chief Psychologist told the OIG that Epstein and his attorney mocked her for thinking Epstein was suicidal.28 On July 16, 2019, at Epstein’s request, the Chief Psychologist met with Epstein during his attorney conference. The Chief Psychologist noted that Epstein did not have any psychological concerns and denied suicidality. The Chief Psychologist noted that she provided Epstein with psychoeducation regarding additional coping strategies. Epstein was educated about routine and emergency procedures to contact Psychology Department staff and reminded of self-help books and audiotapes that are available to him. The Chief Psychologist noted in her clinical contact report that there was no need for follow-up and that Epstein would be seen in the SHU for rounds and monthly SHU reviews. According to the BOP After Action Review submitted by the Southeast Regional Director, the Chief Psychologist’s meeting with Epstein on July 16, 2019, at Epstein’s request during his attorney conference was inappropriate. The Southeast Regional Director wrote in the report that Epstein attempted to “bring his attorneys into the fray regarding the mental health treatment being provided by the institution.” In the After Action Review, the Southeast Regional Director wrote that it was not typical for the BOP to provide psychological intervention in the presence of others, nor was it appropriate for a BOP psychologist to meet with an inmate’s attorney. When asked by the OIG about these findings, the Chief Psychologist stated that the intention was to check on Epstein, not to breach any security. On July 18, 2019, the Chief Psychologist conducted a monthly SHU review and noted that Epstein was unavailable due to a meeting with his legal team and that she would attempt to interview Epstein in the near future to complete his monthly review. As noted previously, at approximately 1:27 a.m. on July 23, 2019, Epste...
45 Also on July 23, 2019, the Staff Psychologist conducted a suicide risk assessment that included a clinical interview of Epstein and a review of Epstein’s medical record, the psychology data system, and a review of the SENTRY database. According to the Staff Psychologist’s report, Epstein denied knowing why he was placed on suicide watch. BOP records state that Epstein recalled getting a drink of water the night prior and then went back to bed. Epstein’s next recollection was hearing himself snoring. The BOP assessment records reflect that Epstein wanted to know why he was on suicide watch and he was informed that he had been found with a string on his neck. The Staff Psychologist noted that it was unclear whether Epstein had placed the string around his neck or if someone else did. Epstein denied current suicidal or self-harm thoughts or ever having these thoughts; denied a history of self-harm and suicide attempts; and denied feeling hopeless and fearing for his safety. Epstein told the Staff Psychologist that he lived to enjoy life and that his future plans included fighting his criminal case and getting back to his normal life. The Staff Psychologist noted that Epstein was to remain on suicide watch for further observation. The Staff Psychologist told the OIG she had advised BOP staff that Epstein would need a cellmate. The Chief Psychologist said she considered three possibilities to explain the July 23 incident: (1) Epstein and/or Inmate 1 were gaming the system to get something they wanted that they were not getting; (2) Epstein, who really was suicidal, had conducted a rehearsal; or (3) Inmate 1 had assaulted Epstein. The Chief Psychologist told the OIG that after Epstein told her he wanted to be housed with the same cellmate he originally said had assaulted him, she began to think that the third possibility (assault by Inmate 1) was less plausible than the other two possibilities, although she did not know for certain. T...
46 concurred with her determination. Epstein was therefore taken off suicide watch and placed on psychological observation, during which time BOP records reflect that he was continuously observed by inmate companions and seen daily by Psychology Department staff. Forensic Psychologist 2 annotated in the Post Suicide Watch Report that the reason for removing Epstein from suicide watch was due to Epstein stating he had no interest in killing himself; he had described having a wonderful life; and Epstein had said it would be crazy to take his own life and he would not do that to himself. Forensic Psychologist 2 told the FBI that following her clinical visit with Epstein on July 24, 2019, she was cautious with Epstein’s case and his self-reporting of what had occurred the previous day. Forensic Psychologist 2 stated that she observed signs of positivity and that Epstein “adamantly denied suicide.” Nevertheless, she was not comfortable taking Epstein off suicide watch and instead opted to place Epstein on psychological observation, which was a step down from suicide watch. Forensic Psychologist 2 told the FBI that “I made the decision with the consent” of the Chief Psychologist and Associate Warden 2, with whom she had consulted. Forensic Psychologist 2 told the FBI that placing Epstein on psychological observation allowed him to possess hygiene products, two novels, attend legal visits, and take showers. It also allowed him to have standard inmate clothing, a flex pen, a toothbrush and toothpaste, soap, and deodorant. However, Forensic Psychologist 2 explained that it was not healthy for inmates to stay on suicide watch for extended periods of time and they are re-evaluated on a day-to-day basis. According to Forensic Psychologist 2’s Post Suicide Watch Report, Epstein expressed a feeling of safety being housed in the psychological observation area rather than the SHU and asked if there was a safer unit for him to be housed. Forensic Ps...
47 his personally owned medical device. BOP records state that Epstein was aware he would be returning to the SHU but reported that he did not feel well due to lack of sleep and other medical concerns. Epstein asked to stay on psychological observation, where he felt safe, for one more night to get some sleep and then return to the SHU with a cellmate the following day. According to BOP records, the Chief Psychologist informed Epstein that he could stay 1 more night and explained that there were no mental health issues precluding him from returning to the SHU the following day. The Chief Psychologist explained to Epstein that he would be placed in a safe situation in the SHU. Epstein again was provided supportive interventions and psychoeducation regarding additional coping strategies. BOP records state that Epstein was somewhat receptive but more concerned with getting phone calls, recreation, and housing placement concerns. On July 30, 2019, according to BOP records, Epstein reported to the Staff Psychologist that he had not slept well, and Epstein discussed how he did not think he would be able to sleep well in the SHU because of the noise. The Staff Psychologist annotated in the clinical contact summary that documentation revealed Epstein had eaten and taken a shower the day prior (July 29) and also had eaten breakfast on July 30. The Staff Psychologist annotated, Epstein did not display indications of disturbed thought process or content and denied current suicidal or self-harm ideation. BOP records further stated that Epstein agreed to immediately report to staff if he began to have suicidal or self-harm thoughts and that Epstein was future- oriented and did not appear to be a danger to himself. The Staff Psychologist noted in her clinical contact report that she had consulted with the Chief Psychologist and that psychological observation of Epstein would be discontinued. According to her clinical contact report, the Staff Psyc...
48 harming others. Epstein also agreed to contact staff immediately if he experienced any suicidal thoughts or psychological distress. Forensic Psychologist 3’s report further stated that Epstein was receptive to her utilization of cognitive behavioral therapeutic techniques. She wrote that there did not appear to be a need for follow-up at the time and Epstein expressed a willingness to self-refer to Psychology Department staff if needed. According to the report, Epstein would continue to be seen during routine SHU rounds and SHU reviews. On August 1, 2019, according to BOP records, BOP Receiving and Discharge staff, who are responsible for processing inmates who enter or leave the facility, notified the Staff Psychologist that the previous day when the U.S. Marshals Service (USMS) had brought Epstein back to MCC New York from court, they had provided a form on which it was noted that Epstein had “suicidal tendencies.” The OIG reviewed the USMS Prisoner Schedule Report for July 31, 2019, as well as the USMS Prisoner Custody Alert Notice that had annotated in the remarks that Epstein had “Mental Concerns: Suicidal Tendencies.” The Chief Psychologist told the OIG that the USMS annotates suicidal tendencies for many inmates if the USMS was aware the inmate was previously on suicide watch. Therefore, the Chief Psychologist said the annotation was not abnormal since Epstein had just come off suicide watch and Epstein may have told the USMS that he had been on suicide watch. Following receipt of this information from the Receiving and Discharge staff, the Staff Psychologist conducted a suicide risk assessment on August 1 that included a review of Epstein’s previous clinical encounters, medical records, and data in the Psychology Department and SENTRY systems. According to the Staff Psychologist’s assessment, Epstein denied stating he was suicidal and was surprised that the form noted that he had suicidal tendencies. The Staff Psychologi...
49 psychoeducation regarding additional coping strategies, to which Epstein was receptive. Epstein was educated on routine and emergency procedures for contacting Psychology Department staff and also reminded of self-help books and audiotapes that are available to him. The Chief Psychologist wrote that Epstein would be seen in weekly SHU rounds and monthly for SHU reviews. The Chief Psychologist told the OIG that the fact that Epstein underwent three suicide risk assessments was unusual.30 30 Upon reviewing a draft of this report, the Chief Psychologist noted that it was not unusual for someone with static risk factors like Epstein to have received multiple suicide risk assessments. According to the Chief Psychologist upon reviewing a draft of this report, what was unusual was the fact that Epstein was in attorney conference “day and night on a daily basis due to his financial resources.” She noted that it was difficult for Psychology Department staff to interview Epstein because he had a right to his attorney visits, which would last throughout the working day.
50 Chapter 5: The Events of August 8–10, 2019, and Epstein’s Death I. Epstein Signs a New Last Will and Testament on August 8 In the weeks following Epstein’s death, multiple media outlets reported that Epstein signed a new Last Will and Testament on August 8, 2019. At least one media organization published a copy of the notarized document showing that it was signed by Epstein and two of his attorneys and notarized on August 8, 2019. Attorney visitor logs from the Metropolitan Correctional Center in New York, New York (MCC New York) confirmed that those attorneys and the notary public visited Epstein on that date. The Office of the Inspector General (OIG) confirmed via court records that the August 8, 2019 will and other probate-related documents were filed in the Superior Court of the Virgin Islands on August 15, 2019. Among the court filings was an affidavit from another attorney who stated that she received the August 8, 2019 will from Epstein. The OIG confirmed via attorney visitor logs that this attorney also visited Epstein at MCC New York on August 8, 2019. The OIG’s investigation and review revealed that MCC New York personnel were unaware that Epstein had changed his will 2 days before he died. The Chief Psychologist said she had heard that Epstein had changed his will from media reporting following his death. The Chief Psychologist did not know if the media reporting was accurate, but she thought that if it were true, it would have been useful information to know because it would have been a red flag. The Staff Psychologist and the Chief Psychologist told the OIG that if Epstein’s attorneys had notified them or the Psychology Department that Epstein had changed his will, such information would have been a factor warranting a review of Epstein’s mental state and Epstein probably would have been placed back on suicide watch or some type of observation. II. Court Order on August 9 Releasing Epstein-Related Documents in Pend...
51 III. Transfer of Epstein’s Cellmate on August 9 to Another Institution and Failure to Replace Him with Another Inmate A. Notice on August 8 of the Impending Transfer of Epstein’s Cellmate on August 9 As noted above, since July 30, consistent with the Psychology Department’s determination that Epstein needed to have a cellmate, Epstein had been housed with Inmate 3, whom the Warden and the Federal Bureau of Prisons (BOP) executive leadership had selected as an appropriate cellmate. At 10:33 a.m. on August 8, 2019, the U.S. Marshals Service (USMS) sent an email to MCC New York personnel assigned to Receiving and Discharge, the area within the Correctional Services Department that is responsible for processing inmates who enter or leave the facility, with the subject “Transfer of Prisoners from NYM [MCC New York] to GEO.”32 The body of the email identified Inmate 3 as one of the prisoners to be transferred and further stated, “Please schedule the transfer for Friday 8/9/19.” At 3:36 p.m. on the same day, the USMS sent a second email to a number of MCC New York personnel, including Associate Warden 2, the Captain, the SHU Lieutenant, the Day Watch Operations Lieutenant, the Day Watch Activities Lieutenant, the Evening Watch Operations Lieutenant, another Lieutenant, and the Special Investigative Services Lieutenant, with the subject “Prisoner Production 08-09-2019.” This email contained two attachments, one of which was the Prisoner Schedule Report for MCC New York for August 9, 2019. The first page of this attachment reflects that Inmate 3 was scheduled to be transferred from MCC New York to GEO (Queens Detention Facility) on August 9, 2019. This attachment also includes the acronym “WAB” within the Destination/Description portion of the document, which MCC New York personnel told the OIG means “with all belongings.” During their OIG interviews, MCC New York staff members further explained that the “WAB” notation meant that Inmate 3 ...
52 Epstein, and he said he told the second attorney that Epstein could not be housed without a cellmate because of his prior suicide attempt. C. Removal on August 9 of Epstein’s Cellmate from MCC New York According to MCC New York reports, including the Daily Log and the Lieutenant’s Log, on August 9, 2019, at approximately 8:38 a.m., Epstein’s cellmate, Inmate 3, was “pre-removed” and transferred out of MCC New York in a routine, pre-arranged transfer. The Daily Log tracks inmate movements throughout MCC New York each day, while MCC New York Lieutenants utilize the Lieutenant’s Log to document the daily activities that took place within the institution during their respective shifts. The Supervisory Correctional Systems Specialist was the supervisor of Receiving and Discharge on August 9, 2019, and was responsible for overseeing all inmate movements in and out of the institution that day. The Supervisory Correctional Systems Specialist verified that Receiving and Discharge would have used the USMS emails sent on August 8, 2019, to coordinate Inmate 3’s transfer out MCC New York, and since Inmate 3 was listed as “WAB” on the USMS emails, that meant he was being transferred from the facility and not coming back. She explained to the OIG that if Inmate 3 had been going to court, as many pretrial inmates held at MCC New York often did, the Daily Log would have reflected “court,” rather than “pre- remove.” Since the Daily Log listed Inmate 3 as “pre-remove,” the Receiving and Discharge personnel who entered the information into the report were made aware that Inmate 3 was being transferred from MCC New York on or before the morning of August 9, 2019. The Supervisory Correctional Systems Specialist told the OIG that the language in the USMS emails (“WAB,” i.e., “with all belongings”) and MCC New York reports (“pre-removed”) made it clear that Inmate 3 would not be returning to the SHU or MCC New York. The OIG also interviewed the Correctiona...
53 D. Failure to Assign Epstein a New Cellmate on August 9 1. Day Watch Staff Actions on August 9 The SHU Lieutenant told the OIG that he worked at MCC New York on August 8, 2019, from approximately 6 a.m. until approximately 2 p.m., and that he was off on August 9, 2019. The SHU Lieutenant, whose shift ended over an hour before the USMS sent the second email regarding Inmate 3’s impending transfer, told the OIG he was not aware that Inmate 3 was scheduled to be transferred out of MCC New York, and therefore he did not notify the Captain that Epstein would require a new cellmate. According to the SHU Lieutenant, as soon as the SHU staff learned that Inmate 3 would be transferred, they should have notified a Lieutenant on duty. The Day Watch Operations Lieutenant and the Day Watch Activities Lieutenant told the OIG that on August 9, 2019, they had oversight of the SHU from approximately 6 a.m. until 2 p.m. due to their position descriptions and because of the SHU Lieutenant’s absence. According to the MCC New York Staff Roster, on August 9, 2019, SHU Officer #1 was listed as Senior Officer Specialist 5. Although SHU Officer #1 is typically the Officer in Charge, another Senior Officer Specialist told the OIG that, in actuality, he was the Day Watch SHU Officer in Charge on August 9 from approximately 6 a.m. until 2 p.m. The Day Watch SHU Officer in Charge said that since he had the most experience and seniority, he was considered by everyone to be the SHU Officer in Charge, which the SHU Lieutenant confirmed. The Day Watch SHU Officer in Charge told the OIG that he knew that Epstein had to have a cellmate. He said that, as a general practice, every inmate who is transferred from suicide watch and/or psychological observation to the SHU is placed with a cellmate. He also confirmed that the SHU Lieutenant had instructed him that Epstein was to be housed with a cellmate at all times. According to the Day Watch SHU Officer in Charge, be...
54 Watch SHU Officer in Charge, he did not select a new cellmate for Epstein because he was not certain that Inmate 3 had been discharged from the institution, although he assumed that Inmate 3 would not return to the SHU. The Day Watch SHU Officer in Charge told the OIG that when his shift ended at approximately 2 p.m., he informed the Evening Watch SHU Officer in Charge and Senior Officer Specialist 5 that, if Inmate 3 did not return to the SHU, Epstein would need a new cellmate upon Epstein’s return from his attorney visit. The Day Watch SHU Officer in Charge said he specifically recalled telling the Evening Watch SHU Officer in Charge, in the presence of Senior Officer Specialist 5, “Make sure this guy gets a bunkie,” to which the Evening Watch SHU Officer in Charge replied, “All right.” The Day Watch SHU Officer in Charge said that, at some point that day, it was likely that he also informed the Day Watch Operations Lieutenant, but he could not specifically recall if he had done so. The Day Watch SHU Officer in Charge told the OIG that a replacement cellmate should have been identified as soon as it was confirmed that Inmate 3 had left the institution. He said a new cellmate could have been reassigned before the 4 p.m. SHU count if it was known that Inmate 3 was not coming back, but the SHU staff members had until Epstein returned from his attorney visit to assign Epstein a new cellmate. According to the Day Watch SHU Officer in Charge, SHU staff definitely should have realized that Inmate 3 was not returning both during the 4 p.m. count and when Epstein returned from his attorney visit later that evening. The Day Watch SHU Officer in Charge told the OIG that Epstein’s daily routine was that he would be with his attorneys in the attorney conference room until approximately 8 p.m., so SHU personnel had time to make a new cellmate assignment. He said all SHU staff members shared the responsibility to find a replacement cellmate and ...
55 The Day Watch Operations Lieutenant and the Day Watch Activities Lieutenant both told the OIG that they did not know Inmate 3 had been transferred out of the facility, despite the fact that both were recipients of the second email the USMS sent on August 8 that included the information about Inmate 3’s impending transfer out of MCC New York on August 9. Rather, the Day Watch Operations Lieutenant and the Day Watch Activities Lieutenant told the OIG that they believed Inmate 3 had been removed from MCC New York for a court appearance. The Day Watch Activities Lieutenant did not recall Inmate 3 departing the institution with all of his belongings or having any conversations with the Day Watch SHU Officer in Charge or anyone else regarding Inmate 3’s departure from MCC New York. According to the Day Watch Activities Lieutenant, he did not know that Epstein was without a cellmate. Other senior officials, including the Warden, Associate Warden 1, and the Captain, were also unaware of Inmate 3’s transfer and the need to assign Epstein a new cellmate. These officials concurred that while all SHU staff and supervisors were responsible for notifying a supervisor in the chain-of-command of the need to assign Epstein a new cellmate, the Day Watch SHU Officer in Charge bore primary responsibility for the notification because he was the SHU Officer in Charge and one of two people who saw Inmate 3 leave the facility with all of his belongings. The Captain told the OIG that since Epstein was in the attorney conference room all day, no one may have even thought about it, and may have only become aware when they put Epstein back in his cell after his attorney visit that evening. The Captain said as soon as the SHU staff became aware that Epstein was without a cellmate, they should have notified the Evening Watch Operations Lieutenant. The Captain said that if he had been informed, he would have taken immediate action to ensure that Epstein was eithe...
56 The Evening Watch SHU Officer in Charge told the OIG that he eventually learned later that evening that Epstein did not have a cellmate. According to the Evening Watch SHU Officer in Charge, after Epstein returned from his attorney visit and placed a telephone call, he escorted Epstein to his cell and saw that Inmate 3 was not there. According to the Evening Watch SHU Officer in Charge, after he realized that Epstein did not have a cellmate, he, Noel, and the Material Handler, all of whom were working in the SHU that evening, talked about Epstein needing a new cellmate. The Evening Watch SHU Officer in Charge said SHU staff could not just put anyone in the cell with Epstein. In his interview with the OIG, the Evening Watch SHU Officer in Charge stated that he called someone (he could not recall who) and notified that person that Epstein did not have a cellmate. OIG interviews did not identify an individual who received such a call or who witnessed the Evening Watch SHU Officer in Charge making it. Senior Officer Specialist 5 told the OIG that on August 9, he worked in the SHU from approximately 8:45 a.m. until 4 p.m. Senior Officer Specialist 5 said when he reported for duty, Epstein was already with his attorneys, Inmate 3 had already left the SHU, and neither inmate returned to the SHU prior to his departure. Senior Officer Specialist 5 told the OIG that he did not know Inmate 3 had been released from MCC New York and that no one told him Epstein would need a new cellmate, including the Day Watch SHU Officer in Charge, the Captain, the SHU Lieutenant, or anyone from the Psychology Department. CO 2 told the OIG that on August 9, he worked in the SHU from 8 a.m. until 4 p.m. CO 2 said he did not recall Inmate 3 departing the SHU that day, and that he was unaware that Epstein needed a new cellmate. The Evening Watch Operations Lieutenant told the OIG that he was the Operations Lieutenant at the MCC on August 9 from approximately 2 p...
57 had left MCC New York. The Acting Evening Watch Activities Lieutenant did not receive the August 8 USMS email regarding Inmate 3’s transfer. The Morning Watch Operations Lieutenant, who was the Operations Lieutenant from approximately 10 p.m. on August 9 until 6 a.m. on August 10, told the OIG that she did not know that Epstein was required to have a cellmate, and that the Captain never spoke with her about this issue. The Captain confirmed that he did not specifically tell the Morning Watch Operations Lieutenant that Epstein needed a cellmate; however, the Captain said he believed that the Morning Watch Operations Lieutenant should have known of the requirement, and she was one of the recipients of the email from the Psychology Department on July 30, 2019, that informed MCC New York staff that Epstein needed to have an appropriate cellmate. The Morning Watch Operations Lieutenant also received the August 8 USMS email notifying MCC New York supervisory staff of Inmate 3’s scheduled transfer out of MCC New York. The Morning Watch Operations Lieutenant told the OIG that if SHU staff knew that Epstein required a cellmate and did not have one, they should have informed her when she visited the SHU at approximately 4 a.m. on August 10, as part of her Lieutenant rounds. The Material Handler said the SHU was not his regular post and he had not attended SHU training, but he had worked in the SHU approximately 10 to 20 times. According to the Material Handler, on August 9 he reported for a voluntary overtime shift from 12 a.m. to 8 a.m. and then worked his regular 8 a.m. to 4 p.m. shift in the warehouse. At some point during the day shift, the Day Watch Operations Lieutenant called and asked the Material Handler if he could work overtime in the SHU, and he agreed. The Material Handler said he worked the 4 p.m. to 12 a.m. shift in the SHU with the Evening Watch SHU Officer in Charge and Noel. The Material Handler told the OIG that he felt p...
58 he did not know that Inmate 3 was removed from MCC New York on August 9, and that Epstein was without a cellmate during his shift on August 10. IV. Epstein is Allowed to Make an Unmonitored Telephone Call on August 9 For safety and security reasons, BOP policy requires that all inmate telephone calls be made through the Inmate Telephone System. BOP records reflect that Epstein placed an unrecorded, unmonitored telephone call to a telephone number in the local 646 area code using a non-Inmate Telephone System line on August 9, 2019, from 6:58 p.m. to 7:19 p.m. No other BOP records exist regarding the unmonitored call, including identity of the person called or a summary of the conversation. The OIG found no evidence that Epstein signed an Acknowledgement of Inmate form, as required by BOP policy and necessary for him to use a non-Inmate Telephone System line. The Acknowledgement of Inmate form provides, among other things, that the BOP reserves the authority to monitor and record non-attorney conversations on any telephone located within the institution to preserve the security and orderly management of the institution and to protect the public. The OIG did not find that any notification was made to the MCC New York’s Special Investigative Services staff advising the telephone call had been made, the date and time of the telephone call, the name of the person being called, Epstein’s name and register number, or a brief statement explaining the purpose of Epstein’s telephone call, as BOP policy requires. The Evening Watch Operations Lieutenant told the OIG that when he was preparing to escort Epstein back to the SHU from the attorney conference room on August 9, 2019, a Unit Manager said to the Evening Watch Operations Lieutenant that he was going to escort Epstein, so he could provide Epstein with the opportunity to place a telephone call using an unrecorded legal telephone line that is utilized by inmates to call their attorneys. T...
59 a part of his job, and he would allow inmates to place telephone calls if they were unable to make calls under ordinary circumstances. The Unit Manager told the OIG that at approximately 6:45 p.m., he and Senior Officer Specialist 1 escorted Epstein from the attorney conference room to the SHU so that Epstein could place a telephone call. The Unit Manager said he put Epstein in the shower area to make the telephone call because COs were present in that area. The Unit Manager explained that he also chose the shower area because that location ensured Epstein would not be able to pull the phone cord into his cell and use it to harm himself. The Unit Manager said he plugged the telephone line into the legal line, which was not recorded, and dialed the telephone number that Epstein provided. As noted above, the number that was dialed was in the local 646 area code. The Unit Manager said he allowed Epstein to place the telephone call on the unrecorded legal line because he believed that Epstein had not set up his Inmate Telephone System account that would have allowed him to call on the institutions recorded lines. According to the Unit Manager, a male answered, and the Unit Manager handed the receiver to Epstein. The Unit Manager heard Epstein say, “Hey, how are you doing? How’s everything?” The Unit Manager admitted that he should have verified who was on the line, as Epstein had requested to make a telephone call to speak with his mother, and it was a male who answered the phone. The Unit Manager said he could not verify the phone number because he believed that Epstein did not have his Inmate Telephone System account set up, and he did not have any phone numbers associated with his account. The Unit Manager told the OIG that after he handed the telephone to Epstein, his shift ended so he left the SHU and left MCC New York for the day. The Unit Manager said that when he left the SHU, Epstein was still on the call and the Evening Wa...
60 telephone call, Epstein told Individual 1 that the press had gotten crazy, and they discussed personal things such as books, music, and hygiene while incarcerated. According to the representations by Individual 1’s counsel, Epstein told Individual 1, “They are trying to keep me safe,” and that his case would take a little longer than he originally thought. He told Individual 1 he loved her, to be strong, and that he would not be able to call her again for another month. Senior Officer Specialist 1 told the OIG that he was not a witness to Epstein’s August 9 call, but he had previously discussed telephone calls with Epstein and knew that Epstein had the requisite paperwork that allowed him to place calls through the Inmate Telephone System. Senior Officer Specialist 1 told the OIG that Epstein was issued the necessary documentation to make telephone calls when Inmate 1 was his cellmate. Senior Officer Specialist 1 also advised the OIG about an interaction that he had with one of Epstein’s attorneys prior to August 9 when he was on an elevator with Epstein and the attorney. According to Senior Officer Specialist 1, Epstein’s attorney asked him about getting Epstein the necessary documentation to make calls. Senior Officer Specialist 1 said he then verified that Epstein was able to make calls through the Inmate Telephone System. When Senior Officer Specialist 1 asked Epstein why he had said he was unable to make calls, Epstein responded, “[T]hey said they monitor those phone calls.” Senior Officer Specialist 1 said that in a subsequent conversation with Epstein’s attorney, the attorney asked how Epstein could get an unmonitored call. Senior Officer Specialist 1 told Epstein’s attorney that decision had to be made by a Lieutenant or Unit Manager. Noel told the OIG that after Epstein’s attorney conference on August 9, the Unit Manager plugged a telephone line in the legal line, and placed Epstein in a shower area within the SHU where h...
61 what happened on that phone call. It could have potentially led to the incident [Epstein’s death], but we don’t, we will never know.” V. Failure to Conduct SHU Inmate Counts and Staff Rounds on August 9–-10 A. SHU Inmate Counts As detailed in the BOP policies section of Chapter 2, the BOP requires COs assigned to guard inmates to conduct institution-wide counts of inmates at regularly scheduled intervals each day to ensure that all inmates are present and accounted for at the appropriate location within the facility. Performing an institutional count is one of the basic and essential aspects of a CO’s job, and the count was one of the basic and essential components of the daily operation of MCC New York. The Captain told the OIG that counts are a core responsibility of COs and ensure accountability of the inmates. The Evening Watch Operations Lieutenant said that it is very important that the institutional count is accurate because that is how staff members know if all inmates are present and if anyone has escaped. On weekdays, MCC New York conducted institutional counts at 12 a.m., 3 a.m., 5 a.m., 4 p.m., and 10 p.m. The 10 p.m. count was a stand-up count, which meant that inmates were required to stand when they were counted. Pursuant to BOP policy and MCC New York SHU Post Orders, two COs were required to perform the institutional count for each housing unit, including the SHU. To perform the institutional count in the SHU, BOP policy and MCC New York SHU Post Orders required two officers to walk from tier to tier to observe and count each individual inmate. During each count, one CO would count the inmates while the other officer observed the inmates. The two officers would then switch roles and compare the count numbers. If the totals did not match, then the officers had to conduct another count in the same manner. COs had to document their performance of inmate counts on an official MCC New York form often referred to ...
62 result, many SHU staff and supervisors were unaware that Epstein did not have a cellmate as the Psychology Department had determined was necessary, and Epstein was alone and unobserved in his cell for an extended period of time. 1. The 4 p.m. SHU Count on August 9 The OIG’s investigation determined that the 4 p.m. SHU inmate count on August 9, 2019, was inaccurate because SHU staff did not physically count the inmates as required by BOP policy and instead relied upon a predetermined number of inmates believed to be in the SHU at that time. However, Epstein, who was in the SHU attorney visitation room, was correctly accounted for during the 4 p.m. and subsequent SHU counts. The OIG determined that the error in the 4 p.m. SHU count was carried over into the next inmate count at 10 p.m. that counted an inmate who had been transferred out of the SHU. The SHU inmate count was not corrected until 12 a.m. when the Morning Watch Operations Lieutenant reviewed the master institutional count and housing unit count slips and informed SHU staff of the correct number of inmates in the SHU at that time. Senior Officer Specialist 5 told the OIG that prior to his departure from the SHU at approximately 4 p.m., he told the Evening Watch SHU Officer in Charge what the SHU count should be. In addition, the Day Watch SHU Officer in Charge told the OIG that SHU staff maintain a “cheat sheet,” which lists the number of inmates believed to be in the SHU at any given time. When interviewed by the OIG, the Day Watch SHU Officer in Charge reviewed the 4 p.m. SHU count slip from August 9, 2019, which was signed by the Evening Watch SHU Officer in Charge and CO Noel. Based on his review, the Day Watch SHU Officer in Charge told the OIG that the Evening Watch SHU Officer in Charge and Noel probably did not count the inmates in the SHU. He said they likely wrote down the numbers they thought should have been entered for the count because the count slip inaccura...
63 count slip.36 During his OIG interview, the Evening Watch SHU Officer in Charge reviewed BOP documents regarding the inmate’s transfer from the SHU and acknowledged further that based on that transfer, the number of inmates listed on the SHU count slip he and Noel submitted for the 4 p.m. count, the count slip was incorrect. Noel admitted in the deferred prosecution agreement she entered into with the U.S. Attorney’s Office for the Southern District of New York that she completed false count slips on August 9 and 10. Noel initially told the OIG that she did not conduct the 4 p.m. count on August 9, but after acknowledging that she signed the 4 p.m. SHU count slip, Noel said she did not recall if she conducted the count. According to Noel, she and other SHU staff filled out the count slip before conducting the counts because they knew the number of inmates they were supposed to report. 2. The 10 p.m. SHU Count on August 9 At the time of the 10 p.m. count, all inmates in the MCC New York SHU, including Epstein, were locked in their cells for the night. At or around that time, the two officers assigned to the SHU were responsible for conducting the 10 p.m. stand up count. At 10 p.m. on August 9, the two assigned SHU officers were Noel and the Material Handler. Through review and analysis of the SHU security camera video, witness statements, and BOP records, the OIG determined that MCC New York staff did not perform the 10 p.m. count in the SHU.37 Nonetheless, Noel and the Material Handler completed and signed the 10 p.m. SHU count slip. The 10 p.m. SHU count slip listed the total number of inmates as “73 + 1.” According to the MCC New York master count sheet for the 10 p.m. count on August 9, 2019, all units had verbally reported their inmate counts to the Control Center by 10:30 p.m.38 At approximately 10:36 p.m., the Control Center completed all paperwork and officially cleared the 10 p.m. institutional count. The Material Handl...
64 documentation shows the count was verbally cleared by the Control Center at 10:30 p.m. It therefore appears that the video depicts Noel conducting a later round in the SHU, as she was required to do every 30 minutes during her shift, and not the 10 p.m. SHU count. Noel said she wrote the 73 on the count slip but she did not remember if she or someone else had written “+ 1” on the count slip and she did not know why “+1” was on the count slip. Noel claimed that, unlike the 4 p.m. count slip, which the Evening Watch Officer in Charge pre-filled, she did not prepare the 10 p.m. count slip in advance of the count. Noel said she did not know that the 10 p.m. SHU count slip, which listed 73 inmates, was inaccurate, and she could not explain why the 12 a.m. count also inaccurately listed that 73 inmates were physically present in the SHU, whereas the 3 a.m. and 5 a.m. count slips accurately listed 72 inmates in the SHU. Senior Officer Specialist 6 told the OIG that on August 9, 2019, he worked in the Control Center from approximately 4 p.m. until 12 a.m., and then he worked as an Internal Officer from 12 a.m. until 8 a.m. on August 10. According to Senior Officer Specialist 6, he took the August 9 10 p.m. institutional count by himself in the Control Center, and assisted with the 12 a.m., 3 a.m., and 5 a.m. counts on August 10 as an Internal Officer. Senior Officer Specialist 6 confirmed to the OIG, as MCC New York records reflect, that he had received verbal counts from all units by 10:30 p.m., and further stated that he had cleared the institutional count at 10:36 p.m., which was when paperwork was complete and the count was officially complete. Senior Officer Specialist 6 reviewed the MCC New York 10 p.m. institutional count, which showed that the SHU had 73 inmates assigned, whereas the Receiving and Discharge Department had zero inmates assigned to the unit. When questioned by the OIG about the 10 p.m. SHU count slip that listed “73 +...
65 Figure 5.1 10 p.m. Count Slips from the SHU and Receiving and Delivery on August 9 Note: The images have been modified for privacy reasons. Source: BOP Senior Officer Specialist 6 did not recall if he wrote on the count slips at the time of the 10 p.m. count or during the 12 a.m. count when Inmate 4 was transferred in SENTRY from the SHU to Receiving and Discharge. Senior Officer Specialist 6 told the OIG that if he had made the notations at the time of the 10 p.m. count, he should not have cleared the count. Instead, he should have created a new master count sheet and requested that the SHU staff conduct a new count, provide a new count slip, and discard the inaccurate SHU count slip. Senior Officer Specialist 6 told the OIG that an Operations Lieutenant would have needed to authorize him to do the “ghost count” and write on the count slips, although he could not recall precisely who gave him the authorization or when he had done so. The OIG investigation and review determined that the only Operations Lieutenant on duty at the time was the Morning Watch Operations Lieutenant, who started her shift at 10 p.m. on August 9. When questioned by the OIG, the Morning Watch Operations Lieutenant adamantly denied having authorized a “ghost count” and the OIG identified no record or witness (other than Senior Officer Specialist 6) to indicate that she had done so. The OIG interviewed other MCC New York personnel, who said “ghost counting” was not permitted, and stressed the importance of an accurate physical count of inmates. 3. The 12 a.m., 3 a.m., and 5 a.m. SHU Counts on August 10 The Morning Watch Operations Lieutenant told the OIG that she supervised the August 10 12 a.m. institutional count from the Control Center. During the count, the Morning Watch Operations Lieutenant said she identified the issue with the inaccuracy of the SHU count slip because it counted Inmate 4 as present in the SHU, when in actuality he had been removed ...
66 Watch Operations Lieutenant told the OIG that she believed she told the SHU staff to conduct a new count and create a new count slip, but she did not know if they had actually done so. During his interview with the OIG, Senior Officer Specialist 6 reviewed BOP records relating to the inmate transfer, the 12 a.m. institutional count, and the housing unit count slips. Based on his review of this material, Senior Officer Specialist 6 said the 12 a.m. SHU count slip was inaccurate because it continued to list 73 inmates instead of the 72 inmates who were physically present in the SHU at that time. Senior Officer Specialist 6 reviewed the institutional counts and SHU count slips for the 3 a.m. and 5 a.m. counts and told the OIG that they were accurate because they listed the SHU as having 72 inmates. At approximately 12 a.m. on August 10, 2019, Material Handler Thomas replaced the other Material Handler, and he and Noel were the only two staff members on duty in the SHU. Noel and Thomas were responsible for conducting the 12 a.m., 3 a.m., and 5 a.m. counts in the SHU. Through review and analysis of the SHU security camera video, witness statements, and BOP records, the OIG determined that Noel and Thomas did not perform any of these counts. Nonetheless, Noel and Thomas completed and signed SHU count slips for each of the three counts, and in reliance on the count slips, the Control Center cleared the 12 a.m., 3 a.m., and 5 a.m. institutional counts at approximately 12:49 a.m., 3:24 a.m., and 5:30 a.m., respectively. Noel and Thomas both admitted to the OIG that they did not conduct the 12 a.m., 3 a.m., and 5 a.m. counts on August 10, and that they had falsified the respective count slips. Noel told the OIG that she signed the August 10 12 a.m., 3 a.m., and 5 a.m. count slips that Thomas had prefilled. Noel said she did not know why the 12 a.m. count slip documented that there were 73 inmates in the SHU, whereas the 3 a.m. and 5 a.m. slip...
67 Thomas acknowledged that neither he nor Noel conducted any rounds or counts in the SHU during their shift between approximately 12 a.m. and approximately 6:30 a.m. Thomas said the August 10, 2019 round sheets were signed, but the rounds were not conducted because he was tired that day. Thomas recalled “dozing off from here and there” during his shift, but he did not know if Noel slept. Thomas did not recall having a conversation with anyone concerning the discrepancy between the 12 a.m. SHU count slip, which listed 73 inmates, and the institutional count, which listed 72 inmates in the SHU. Thomas said he had filled out and signed the 3 a.m. SHU count slip, which listed 72 inmates in the SHU. Thomas did not know why the number of inmates was different on the 12 a.m. and 3 a.m. count slips and did not recall speaking with the Morning Watch Operations Lieutenant about the 12 a.m. count. Thomas told the OIG that he knew he was falsely certifying the count slips when he signed them on August 10, 2019. B. Staff Rounds in the SHU 1. CO Rounds As detailed in the BOP Policies section of Chapter 2, in addition to inmate counts, BOP policy and MCC New York SHU Post Orders required that COs assigned to the SHU conduct rounds to observe all inmates at least twice an hour. As part of their assigned duties, MCC New York SHU officers had to walk each of the tiers of the SHU twice an hour on an irregular schedule, once during the first 30 minutes and again during the second 30 minutes, with both rounds occurring no more than 40 minutes apart. COs working in the SHU were required to complete and initial an official MCC New York form, often referred to as a “round sheet,” which was reviewed and signed by a supervisor, documenting the date and time of each 30-minute round in each tier of the SHU.40 The Day Watch SHU Officer in Charge told the OIG that SHU staff spoke about conducting rounds on Epstein every day. He said that the Warden, Lieutenant...
68 The Evening Watch SHU Officer in Charge told the OIG that Noel filled out the round sheet on behalf of everyone who was working in the SHU during his shift. The Evening Watch SHU Officer in Charge was not certain if all of the rounds were actually conducted. The Material Handler said he believed the rounds listed on the round sheet as having occurred between 4:01 p.m. to 7:36 p.m. probably had been done, but he was uncertain about the remaining rounds. The Material Handler said he had seen officers “blow off” 30-minute rounds in the past. Noel told the OIG that, as a general practice, when the COs went to the various SHU tiers to distribute food or supplies, they counted that as a round. Noel said she was aware that she was supposed to conduct two rounds every hour during their shift, but that she had never actually completed rounds every 30 minutes while working in the SHU. When asked which rounds she conducted on August 9, 2019, Noel responded, “That’s hard for me to tell because I didn’t conduct it every 30 minutes. It was give out food, pick up the trays, give out toilet paper, go down. So those were the rounds I conducted.” Noel verified that her initials were on the round sheets for August 9 and 10, 2019, and said, consistent with her usual practice, she filled out the round sheets and initialed the round sheets at the start of the 4 p.m. and the 12 a.m. shifts. Noel and Thomas both admitted to the OIG that they did not conduct any of the rounds reflected on the SHU Round Sheet on August 10, 2019, from 12 a.m. until Epstein was found hanged in his cell at approximately 6:30 a.m. Nonetheless, Noel completed and signed more than 75 separate 30-minute entries stating that she and Thomas had, in fact, conducted such rounds.41 Through review and analysis of the SHU video footage, witness statements, and BOP records, the OIG determined that Noel and Thomas did not enter the tiers in the SHU to conduct any of the rounds ...
69 Station. Noel said that during her shift on August 10, 2019, no one went to Epstein’s cell and no one other than the Morning Watch Operations Lieutenant and CO 3 came into the SHU. Through review and analysis of the SHU video footage, witness statements, and BOP records, the OIG determined that at approximately 10:40 p.m. a CO, believed to be Noel, carried linen or inmate clothing up to the L Tier, which was the last time any CO approached the only entrance to the SHU tier in which Epstein was housed. 2. Lieutenant Rounds BOP policy requires that a Lieutenant visit the SHU during each shift to ensure that all procedures are being followed. BOP training for new Lieutenants instructs that the Operations Lieutenant must visit the SHU at least once per shift and “[t]his visit will be substantially more than just entering the unit, signing the log book, and talking with staff.” Additionally, when the SHU Lieutenant is unavailable, the Operations Lieutenant should make rounds in the SHU on each shift. The training instructs that while in the SHU the Operations Lieutenant must walk each range (tier), inspect logs and records, observe activities, and periodically observe SHU inmate counts. The training further outlines that the SHU Lieutenant is responsible for the direct supervision of the unit, including enforcement of rules, review of paperwork, coordination of activities, movement of inmates, and cell searches. The SHU Lieutenant should make rounds on the ranges (tiers) each day. The statements of multiple witnesses were consistent with BOP training materials. The Northeast Regional Director, the Warden, Associate Warden 1, the Captain, and the Day Watch SHU Officer in Charge all told the OIG that Lieutenants should have walked down all of the SHU tiers when conducting a Lieutenant round in the SHU. Noel said the SHU Lieutenant walked the tiers all the time, however, other Lieutenants did not always walk down the tiers. Multiple wit...
70 because he did not conduct any rounds within the SHU on August 9 and he did not recall signing the form. The Morning Watch Operations Lieutenant confirmed that she conducted her round in the SHU at approximately 4 a.m. on August 10. The Morning Watch Operations Lieutenant said she went up to the 10 South Unit and then back down to the SHU because she needed to sign the round sheets. Contrary to BOP training for new Lieutenants, which she attended in 2011, the Morning Watch Operations Lieutenant told the OIG, “We are not required to go to each individual cell and look at the inmates. When we make rounds, we get with the officers.” The Morning Watch Operations Lieutenant said she did not conduct a round to observe the inmates when she visited the SHU. Noel confirmed that the Morning Watch Operations Lieutenant visited the SHU but did not walk down the tiers. Through review and analysis of the SHU security camera video, witness statements, and BOP records, the OIG determined that at approximately 4 a.m. on August 10, 2019, the Morning Watch Operations Lieutenant briefly visited the SHU as part of her supervisory duties and conferred with Noel and Thomas, who were seated at and around the SHU Officers’ Station in the common area of the SHU. Noel told the OIG that at approximately 5:30 a.m., Thomas went to the 10 South Unit, which was adjacent to the SHU, to relieve CO 3, and that CO 3 briefly walked through the SHU common area as he left and returned from his break. The OIG’s review and analysis of the video footage revealed that, aside from those two officers, no one entered the SHU and no one conducted any counts or rounds. VI. Epstein’s Death on August 10 A. Discovery of Epstein Hanged in Cell and Emergency Response On August 10, 2019, shortly after 6 a.m., the doorbell to the SHU rang, indicating that a delivery of breakfast carts had arrived at the SHU. Noel and Thomas retrieved the breakfast carts from the double-locked entr...
71 Thomas explained that when he first entered Epstein’s cell, Epstein had an orange string, presumably from a sheet or a shirt, around his neck. The end of the string was tied to the top portion of the bunkbed. Epstein was suspended from the top bunk in a near-seated position, with his buttocks approximately 1 inch to 1 inch and a half off the floor and his legs extended out straight on the floor. Thomas said Epstein did not look discolored or very different from when he last saw Epstein alive. Thomas said he immediately ripped the orange sheet or shirt away from the bunkbed, and Epstein’s buttocks dropped approximately 1 inch to 1 inch and a half to the ground. Thomas then lowered Epstein’s entire body to the floor and, because he did not believe Epstein was breathing, Thomas immediately began providing chest compressions until responding MCC New York staff members arrived approximately 1 minute later. Thomas said he did not provide rescue breaths and was unaware if Epstein was dead or alive because he never checked for a pulse before initiating chest compressions. Thomas said medical personnel took over the emergency response, including chest compressions and use of an automated external defibrillator (AED), when they arrived. Thomas said he assisted with bringing Epstein down to the Health Services Unit on the second floor, and that he left MCC New York at approximately 8 a.m. Thomas said he had received cardiopulmonary resuscitation (CPR) training during MCC New York annual refresher training and had responded to medical emergencies in the past, but this was the first time he was the first responder. Thomas said he was present in the SHU for his entire shift on August 10, 2019, from 12 a.m. until the time he attempted to deliver breakfast to Epstein at approximately 6:30 a.m. and did not see anyone go inside Epstein’s cell during his shift. Thomas said that he would have known if someone went in or out of Epstein’s...
72 and then she heard Thomas rip something. Noel said she observed Thomas lifting Epstein from under his arms and dragging him back out of the corner of the cell and laid him down on the ground to perform CPR. According to Noel, within seconds of Thomas calling out for the cutter she hit the body alarm, which is a button on an MCC staff member’s radio that is used to signal distress or an emergency. Noel recalled hearing Thomas say, “Breathe, Epstein, breathe,” and “We’re going to be in so much trouble.” Noel said she stood at the door about a foot away from Epstein’s cell and never went in. Noel said Thomas only performed chest compressions and said she did not see Thomas checking for breath or pulse. Noel said that when she saw Epstein, he looked blue and did not have a shirt on or anything around his neck. Noel said she did not get the cutter because Thomas did not need it based upon the ripping sound she heard. Noel said an MCC New York Lieutenant who responded to the alarm asked her what happened, and before she got the chance to answer, Thomas stated, “Oh, it’s not her fault, we fucked up.” Noel did not recall making any comments or statements to the Lieutenant. Other than the Lieutenant, Noel did not recall which COs responded to the alarm and she did not know what happened in the cell after MCC New York staff arrived because she was waiting at the bottom of the steps outside the L Tier. Noel said she was alone in the SHU for 20 minutes after they left with Epstein and she kept calling the Control Center to get status updates. Noel told the OIG that Epstein’s cell was approximately 15 feet from the SHU Officers’ Station. Noel said she would have known if someone went in or out of Epstein’s cell overnight and no one did. She also said that there was no indication that any of the inmates could have gotten out of their cells. Noel said she never slept during her shift on August 9-10, 2019. Noel said that when she is seen on ...
73 then returned to the SHU and worked there for approximately 1 hour, along with the Morning Watch Operations Lieutenant and Noel. The Electronics Technician believed he was in the SHU prior to 7 a.m. and until approximately 8 a.m., but he was not positive with regard to the times. The Electronics Technician said he delivered food to the inmates on one tier while the Morning Watch Operations Lieutenant did the same on another tier while Noel unlocked the doors outside of the tiers for the Electronics Technician and the Morning Watch Operations Lieutenant. The Electronics Technician said that when they were delivering food to the inmates, he heard the inmates saying, “You killed him. You weren’t making rounds. You killed him.” The Electronics Technician told the OIG that the inmates also said Thomas and Noel just sat at the SHU Officers’ Station and never checked on the inmates. The Electronics Technician told the OIG he understood the inmates to be saying that Thomas and Noel were responsible for Epstein’s death because they had not conducted rounds during their shift. The Electronics Technician said he believed that Epstein took his own life and said he had no reason to believe otherwise. Senior Officer Specialist 6 said he responded to the emergency call at 6:33 a.m. and when he arrived, staff members were already performing CPR on Epstein. Senior Officer Specialist 6 said he assisted with transporting Epstein to the Health Services Unit, taking Epstein to the ambulance, and then followed the ambulance to the hospital in another vehicle, and stayed at the hospital until he was relieved from duty. The OIG also reviewed photographs that were taken in the MCC New York Health Services Unit of EMTs attempting to resuscitate Epstein. The photographs show, among other things, Epstein on his back with an intravenous line in his arm, his orange BOP-issued shirt ripped open and laying around his arms, and him wearing orange BOP-issued boxe...
74 revive Epstein. Epstein was not responsive. Inmate 5 said Epstein looked dead when the male CO tried to pick him up and they both fell. Inmate 5 said officers had trouble getting Epstein onto the stretcher because Epstein was basically dead weight. When the officers did get Epstein on the stretcher, Epstein still had on headphones.44 Inmate 5 did not see any marks around Epstein’s neck, and he did not see a rope around Epstein’s neck. However, Inmate 5 saw a male CO come out of Epstein’s cell with a sheet that had a loop and knot. Figure 5.4 Location of the Cells Assigned to Inmates 5-7 in Relation to Epstein’s Cell in the L Tier Source: DOJ OIG schematic drawing depicting the MCC New York SHU Inmate 6 told the OIG that on August 9 and 10, 2019, he was housed within the SHU on L Tier in a cell directly across from Epstein’s cell. Inmate 6 last saw Epstein’s cellmate, Inmate 3, on August 9 when Inmate 3 said, “See you later. I’m going to court.” Inmate 6 said Inmate 3 did not return that night and said the SHU officers never conducted their required 30-minute rounds. Inmate 6 believed the COs last checked on the inmates in the SHU on August 10 between 12:30 a.m. and 1 a.m. Inmate 6 did not observe anyone entering Epstein’s cell after Epstein returned from his legal visit on August 9, 2019; did not hear noise that night; and said Epstein’s door was not opened during the night. Inmate 6 said a male officer discovered Epstein dead during breakfast delivery on August 10. Inmate 6 said he observed the male CO entered Epstein’s cell and began performing CPR, while the female CO, who appeared panicked, stayed outside of the cell. Inmate 6 said he observed Epstein on the floor but did not see a rope over Epstein’s head. However, when Epstein was removed from his cell, Inmate 6 observed the COs holding a rope and a 44 An MP3 player with headphones was obtained as evidence by the Federal Bureau of Investigation (FBI).
75 defibrillator. Inmate 6 did not see marks on Epstein’s neck but did see bruising on his face and observed earphones that were still in place on Epstein’s ears. Inmate 7, who was two cells down from Epstein’s cell and on the other side of the tier, told the OIG that he could not see into Epstein’s cell but he could see the cell door. Inmate 7 said that after dinner was brought to Epstein’s cell on the evening of August 9, 2019, Inmate 7 did not recall seeing anyone going in or out of Epstein’s cell until the following morning at around 6 a.m. He further stated that he did not hear any door “pop open” that evening. Inmate 7 said he remembered waking up around 6 a.m. on August 10, 2019, and hearing a voice, possibly male, saying “Breathe.” Inmate 7 said he saw Epstein removed from his cell on a stretcher. In addition, the OIG and the Federal Bureau of Investigation (FBI) interviewed seven inmates assigned to other tiers in the SHU, none of whom had any direct knowledge of how Epstein died. These inmates consistently reported that the SHU officers did not systematically conduct the counts and rounds as required on the evening Epstein died and that the last round was either between 9:30–10 p.m. or 12:30– 1 a.m. Several inmates told the OIG that before Epstein died the SHU staff never conducted rounds at night. According to the BOP Form 583 Report of Incident, on August 10, 2019, at approximately 6:33 a.m., while delivering the breakfast meal, Epstein was found unresponsive in his cell. Consistent with the required response to a suspected suicide outlined in the MCC New York General Housing Unit Post Orders that are described in Chapter 2, staff called for assistance and began life-saving measures.45 At 6:39 a.m., Epstein was taken to the MCC New York Health Services Unit, and Emergency Medical Services (EMS) arrived to MCC New York at 6:43 a.m. Epstein was transported to the local hospital, New York Presbyterian Lower Manhattan Hospit...
76 According to a memorandum attached to the Form 583 from the Correctional Systems Officer dated August 10, 2019, after Noel called the medical emergency, the Correctional Systems Officer received a call from staff in the SHU instructing her to call 911 for an ambulance. The Correctional Systems Officer notified the New York Police Department (NYPD) via the MCC New York institutional NYPD telephone. The Correctional Systems Officer then informed NYPD that MCC New York needed an ambulance and medical assistance for one of the inmates. The New York City Fire Department and EMS arrived at MCC New York at 6:43 a.m. and were escorted to the second-floor medical area. EMS departed MCC New York with Epstein and a BOP escort via ambulance and chase car to the local hospital at 7:10 a.m. The Morning Watch Operations Lieutenant told the OIG that she was relieved as the Operations Lieutenant prior to 6 a.m. on August 10, 2019, but was still working on things like the Daily Activity Reports and Lieutenant Logs that she did not get to finish during her shift. At some point, the Morning Watch Operations Lieutenant heard that there was a medical emergency in SHU, so she went to assist because she knew that inmates would need to be given food and other things would need to be done. The Morning Watch Operations Lieutenant estimated that she went to the SHU around 7 a.m. to help with the inmate meals, and believed the Electronics Technician was also helping out. Noel was there, but she was not helping with delivering food to the inmates. The Morning Watch Operations Lieutenant said that after the meals were delivered, she finished up and went home. All MCC New York staff members who were interviewed by the OIG said they did not know of any information suggesting that Epstein’s cause of death was something other than suicide. Additionally, no inmate provided the OIG with information suggesting that anyone assisted Epstein with taking his own life or ...
77 Photograph of a Piece of Orange Cloth Tied into a Noose Recovered from Epstein’s Cell After His Death47 the search was not of Epstein’s cell.48 BOP records did not indicate when Epstein’s cell was last searched. The Day Watch SHU Officer in Charge told the OIG that at least five cell searches should be conducted on the day and night watch shifts within the SHU, and that cell searches are conducted in cells every time the inmate departs the cell. He said the SHU Officer in Charge was responsible for making sure the searches were conducted and logged into the BOP TRUSCOPE database. The Day Watch SHU Officer in Charge said that only one cell search was entered into TRUSCOPE on August 9, 2019, because cell searches were tedious to enter, and he was busy. He did not believe that it was a problem that only one cell search was logged on August 9 because he said the SHU staff would have gone into every cell when the inmates took their showers. He said that during the period of Epstein’s custody, SHU inmates showered on Mondays, Wednesdays, and Fridays. The Day Watch SHU Officer in Charge said that during showers, SHU staff searched every cell. He explained that all of the SHU cells should have been searched on Friday, August 9 because it was a shower day. He said SHU staff should also conduct cell searches when inmates go to the recreation area or for attorney visits. According to the Day Watch SHU Officer in Charge, Epstein’s cell should have been searched because both Epstein and Inmate 3 left the cell on the morning of August 9. He further stated that he believed that the majority of cells in the SHU were searched although, as noted above, the SHU staff logged only one cell search in TRUSCOPE on August 9 and the search was not of Epstein’s cell. 47 As noted previously, Epstein’s cell contained an excessive amount of linens, some of which had been ripped into thin strips and tied like a noose. Figure 6.5 depicts one such noos...
78 The Day Watch SHU Officer in Charge told the OIG that in August 2019, each inmate would have been authorized to have two sheets and one blanket. He said that in the winter, inmates are allowed to have an additional blanket. When interviewed by the OIG, the Day Watch SHU Officer in Charge reviewed a picture of Epstein’s cell from August 10, 2019, after Epstein had been removed from the cell. The Day Watch SHU Officer in Charge said there appeared to be an excess number of linens and blankets in the cell, which he believed were for both Epstein and Inmate 3, and that there were possibly a couple of extra sheets as well. He noted that there were two mattresses in the cell and deduced that Inmate 3’s assigned items had not yet been removed even though he had departed MCC New York earlier that day. According to the Day Watch SHU Officer in Charge, Inmate 3’s items should have been removed as soon as the SHU staff knew Inmate 3 was not returning. He told the OIG that any extra linens or blankets should be removed when the inmates take showers and their cells are searched. He told the OIG that he believed the purpose of limiting the linens provided to the inmates was to ensure there was enough to go around and that it was more of an administrative matter rather than a security matter. The Captain also reviewed the picture of Epstein’s cell from August 10, 2019, when interviewed by the OIG. He said Epstein had too many linens, t-shirts, and blankets in his cell. The Captain said the SHU staff were responsible for removing those items because they did not want to hear the other inmates complain that they were not issued the same number of items. The Captain stated that it is also a security issue because it “gives the inmates the materials to be able to make homemade fashioned and improvised nooses” or “use it as escape paraphernalia,” such as a rope that inmates had used to escape from another facility in Chicago. Inmate 3 ...
79 following suicide watch and psychological observation, Inmate 3 asked Epstein not to kill himself while Inmate 3 was his cellmate because Inmate 3 had a chance to go home soon. In response, Epstein told Inmate 3 not to worry and that he was not going to cause him any trouble. When Inmate 3 left on August 9, he told Epstein that he would leave the clothesline in the cell so that Epstein could wash his clothes. Inmate 3 did not say anything about a noose having been in the cell, but he said there were five blankets in their cell when he left. C. Autopsy Results On August 11, 2019, the Office of the Chief Medical Examiner, City of New York, performed an autopsy on Epstein and determined that the cause of death was hanging and the manner of death a suicide. One of the office’s Medical Examiners performed the autopsy, and the autopsy report was reviewed by the First Deputy Chief Medical Examiner. In connection with this investigation, the OIG interviewed the Medical Examiner who performed the Epstein autopsy (hereinafter the “Medical Examiner”). The Medical Examiner told the OIG that the pattern of Epstein’s neck bone fractures was consistent with a hanging. The Medical Examiner explained that a different fracture pattern is present if there has been a manual compression of the neck versus a sustained pressure like in a hanging, and the pattern of Epstein’s neck fractures was that of a hanging. The Medical Examiner also said Epstein had petechial hemorrhages, which are pinpoint bleeds in skin, on his face and mouth. These hemorrhages are caused when the blood flow is obstructed and the small skin capillaries burst. The Medical Examiner additionally identified plethora, which is purple discoloration of the skin, and stated that both petechial hemorrhages and plethora are consistent with suicide by hanging. The Medical Examiner stated that Epstein’s petechia and plethora were identified from his neck up. In homicidal strangulations, ...
80 independent medical judgment and that the Medical Examiner was not pressured or otherwise subjected to any attempt to influence her ruling.
81 Chapter 6: The Availability of Limited Recorded Video Evidence Due to the Security Camera Recording System Failure In August 2019, the Metropolitan Correctional Center located in New York, New York (MCC New York) had approximately 150 video security cameras (no audio) placed throughout the institution. The Office of the Inspector General (OIG) found that approximately 11 cameras were located in and around the Special Housing Unit (SHU) where Epstein was confined at the time of his death on August 10, 2019, including one at the end of the L Tier where Epstein was housed that showed any movement in or out of inmate cells and in the Tier’s hallway. In addition to broadcasting live video, MCC New York had a system that recorded the live video feeds. Following Epstein’s death, MCC New York officials and Federal Bureau of Investigation (FBI) investigators attempted to review video recordings related to the incident and discovered that, although the security cameras were working and transmitting live video, recorded video from most of the cameras in the SHU area was not available due to a malfunction of the video recording system that had occurred on July 29, 2019, including video from the camera at the end of the L Tier. As a result, while the L Tier video camera was transmitting a live video feed on the night of August 9, 2019, and morning of August 10, 2019, the video was not being recorded. One of the cameras that had available recordings from August 9 and 10 was a camera located outside a housing unit adjacent to the SHU. That camera captured video of a large part of the common area of the SHU, including the SHU Officers’ Station and portions of the stairways leading to the different SHU tiers, including the L Tier. Thus, anyone entering or attempting to enter the L Tier from the common area of the SHU, including on August 9 and 10, would have been picked up by the video recorded by that camera. In addition, the recordings showed th...
82 The Electronics Technician told the OIG that, throughout his tenure at MCC New York, the camera system was subject to frequently recurring failures, particularly with respect to the DVR hard drives.49 The Warden, who assumed his responsibilities at MCC New York in May 2018, told the OIG he was generally aware that there were problems with the security camera system throughout the institution. He further stated that efforts were undertaken to determine which cameras were working and which needed to be fixed, and that MCC New York officials intended to ultimately seek funding to replace the entire system. Federal Bureau of Prisons’ (BOP) records reflect that on September 6, 2018, the Warden submitted a memorandum to the BOP’s Northeast Regional Director to request $800,000 in funding to replace the entire camera system. The memorandum identified an estimated project start date of December 1, 2018, and an estimated completion date of February 9, 2019. The BOP approved the funding request, and on September 21, 2018, a contract in the amount of $698,108.99 was awarded to Company 1 to provide various equipment for the project and associated labor. On September 24, 2018, a separate contract in the amount of $34,089.28 was awarded to Company 2 to provide assorted networking equipment and wiring needed to install the camera system. As the camera upgrade project was beginning, BOP officials recognized that MCC New York’s mechanical, electrical, and plumbing systems were also in need of major repairs. MCC New York did not have enough qualified technicians on staff to complete both the camera installation and other repairs needed at the facility, so beginning the week of March 17, 2019, the BOP’s Northeast Regional Office arranged for technicians from other BOP institutions to conduct temporary duty (TDY) assignments at MCC New York to perform the work. During the course of the TDY rotations, work was not consistently conducted on the camera u...
83 recorded video was available for several of the institution’s cameras, so she reported the matter to the Communications Office, and the Electronics Technician arrived to assess the problem sometime before his shift was scheduled to end. The Electronics Technician told the OIG that he found that roughly half of the institution’s approximately 150 cameras, which were assigned to record to DVR 2, were displaying a live video feed but were not recording. The Electronics Technician told the OIG that, before Epstein’s death, no one was specifically tasked with ensuring that video from the cameras was being recorded. The Electronics Technician said he therefore did not perform any daily checks to ensure that video was being recorded. The Warden indicated that SIS staff are usually responsible for checking the system for recording functionality and reporting any problems to the Communications Office. However, the SIS Lieutenant told the OIG that it was her belief that the Electronics Technician should have been checking the system daily to ensure it was recording. The OIG found that there are no BOP policies that specifically state that institutional staff must perform periodic checks to ensure the camera system is fully functional or that security camera systems have the capacity to record.50 The Facility Manager told the OIG that since Epstein’s death, he now checks to ensure that all cameras and the recording system are working on a daily basis, and he subsequently provides a report about the status of the system to the facility’s executive staff, the SIS, and the electronics technicians. B. Response on August 8 and 9 to Discovery of the Recording Failure On August 8, following discovery of the recording failure, Company 1 service request records reflect that the Electronics Technician contacted a Company 1 technical support representative, who ultimately determined that two hard drives within DVR 2 had failed. According to the Electroni...
84 the SIS Lieutenant assumed that the Electronics Technician would remain at the institution after his shift ended that day to correct the issue. The Electronics Technician told the OIG there must have been some miscommunication because he did not say he was going to work overtime and resolve the problem that same evening since he knew the problem could not be fixed in one evening. The Electronics Technician told the OIG that, in hindsight, he should have stayed at the institution to begin work on the problem that same day. The SIS Lieutenant told the OIG that she verbally informed the Captain on August 8 that the cameras were down, but BOP records reflect that the Captain left the institution before the malfunction was discovered. The Captain told the OIG that he did not learn about the DVR recording issue until after Epstein’s death on August 10 when he asked to see video related to the Epstein incident. Associate Warden 1 confirmed she was with the SIS Lieutenant on August 8 when the camera problem was discovered, but she told the OIG she only knew video could not be replayed. She did not know the recording system for certain cameras was down. She could see live video from the cameras on that date, and therefore assumed they were recording. According to the Electronics Technician, after he reported to work on August 9, 2019, and attended to other matters throughout the day, the Electronics Technician obtained the replacement hard drives and attempted to perform the repair sometime late in the day. However, the Electronics Technician told the OIG that no SIS staff were present at that time to give him access to the room in which the DVR room was located, so he requested access from the only other individual who had a key to the space, Correctional Officer (CO) 4.52 According to the Electronics Technician, CO 4 denied him access to the room because CO 4’s shift was ending at 4 p.m., and CO 4 was unable to stay and accompany him in t...
85 Only two cameras in the vicinity of the SHU area were recording to DVR 1 at the time of Epstein’s death.53 One camera was located on the upper-level entrance to the 10 South Unit, a housing unit adjacent to the SHU, near the door MCC New York staff referred to as the “46 door.” That camera captured video of a large part of the common area of the SHU, including the SHU Officers’ Station and portions of the stairways leading to the different SHU tiers, including the tier containing Epstein’s cell. Thus, anyone entering or attempting to enter the L Tier from the common area of the SHU on August 9 and 10 would have been picked up by the video recorded by that camera. Epstein’s cell door, however, was not in that camera’s field of view. The other camera that was recording was located in one of the ninth floor’s two elevator bays and provided video of the ninth-floor fire exit and two of the floor’s four elevators. The available video showed that at approximately 7:49 p.m. on August 9, Epstein was escorted toward the L Tier stairway by an individual believed to be the Evening Watch SHU Officer in Charge.54 At approximately 10:39 p.m., an unidentified CO appeared to walk up the L Tier stairway, and then reappeared within view of the camera at 10:41 p.m. This is believed to be the last time anyone entered L Tier before approximately 6:30 a.m. on August 10. Between approximately 10:40 p.m. on August 9 and just before 6:30 a.m. on August 10, the OIG did not observe on the recorded video any CO or other individual enter any of the SHU tiers, which is consistent with CO Tova Noel and Material Handler Michael Thomas’s admissions to the OIG that the SHU rounds and counts were not conducted during that time frame. At approximately 6:28 a.m., an unidentified officer was observed on the L Tier stairway, presumably to deliver breakfast food trays. Between 6:28 a.m. and 6:32 a.m., an unidentified officer, believed to be Noel, moved back and forth se...
86 Figure 6.1 SHU Camera Locations and Recording Status on August 10, 2019 Source: DOJ OIG schematic drawing depicting the MCC New York SHU Upper Tiers 8 Streaming and Recording Camera Lower Tiers 8 Streaming but not Recording Camera
87 Figure 6.2 Location of Recording SHU Camera at 10th Floor-South entrance Note: The photograph has been modified for privacy reasons. Source: DOJ OIG photograph and DOJ OIG schematic drawing depicting the MCC New York SHU
88 Figure 6.3 Field of View of the SHU Camera at 10th Floor-South Entrance Source: DOJ OIG schematic drawing depicting the MCC New York SHU and the BOP
89 Figure 6.4 Partial View of L Tier Stairway, from the SHU Camera at 10th Floor-South Entrance Source: DOJ OIG and the BOP
90 Figure 6.5 View of SHU Officers’ Station from the SHU Camera at 10th Floor-South Entrance Source: DOJ OIG and the BOP
91 Figure 6.6 Field of View of the Recording 9th Floor Elevator Bay Camera Source: DOJ OIG schematic drawing depicting the MCC New York SHU and the BOP
92 Figure 6.7 Location of Non-Recording Camera in the L Tier of the SHU Source: DOJ OIG schematic drawing depicting the MCC New York SHU and the Office of the Chief Medical Examiner, City of New York The Warden, who was not scheduled to work on August 10, 2019, arrived at the institution later that morning after being notified of Epstein’s death and was informed that most of the cameras in the SHU were not recording. He told the OIG that when the SIS Lieutenant arrived at the facility that morning, he informed her that the SHU cameras had not been recording, and the SIS Lieutenant explained that the hard drive issue had been detected on August 8. He told the OIG that prior to August 10, he was unaware that the DVR 2 issue had been detected on August 8, and that approximately half of the facility’s cameras, and in particular the cameras in the SHU, were found to not be recording on that date. The Electronics Technician told the OIG that the Warden had instructed Electronics Technician to try and recover any potential SHU video that may have been recorded by the cameras assigned to the malfunctioning DVR 2 system, but the Electronics Technician was unable to find anything. The Electronics Technician further said that the Warden wanted to have all the facility’s cameras recording again as soon as possible, so he instructed the Electronics Technician to begin repairing DVR 2. D. FBI Forensic Analysis of the DVR System FBI evidence documents revealed that on August 10, 2019, the FBI seized all hard drives contained within the DVR 2 system. On August 14, 2019, the FBI returned to MCC New York and seized additional DVR 2 components. On August 15, 2019, the FBI seized the entire DVR 1 system.
93 The FBI’s Digital Forensics Analysis Unit in Quantico, Virginia, received MCC New York’s DVR system on August 16, 2019, and began to conduct a forensic analysis of the system. According to FBI forensic reports, DVR 2 did not start successfully. The Digital Forensics Analysis Unit found that the system contained three faulty hard drives. The FBI forensic reports state that the three drives were repaired by an FBI Advanced Data Recovery Specialist, but the DVR was never able to be assembled successfully. The forensic reports further state that an FBI computer scientist and the Company 1 Technician reviewed the DVR 2 controller logs and found that there had previously been “catastrophic disk failures” and no recordings would have been available after July 29, 2019. When the OIG asked the Electronics Technician about this finding by the FBI, he told the OIG he was unaware that cameras were not recording to DVR 2 between July 29 and August 8, 2019. Neither the Warden nor the SIS Lieutenant was aware the cameras assigned to DVR 2 had not been recording since July 29, 2019. The Company 1 Technician could not recall working with the Electronics Technician on any DVR issues prior to August 8, 2019, but he said that if the entire DVR 2 server went down on July 29, 2019, no video would have been able to have been retrieved from that point forward from any of the cameras recording to DVR 2.
94 Chapter 7: Conclusions and Recommendations I. Conclusions Our investigation and review of the Federal Bureau of Prisons’ (BOP) custody, care, and supervision of Jeffrey Epstein identified numerous and serious failures by employees of the Metropolitan Correctional Center located in New York, New York (MCC New York), including falsifying BOP records relating to inmate counts and rounds and multiple violations of MCC New York and BOP policies and procedures, which compromised Epstein’s safety, the safety of other inmates, and the security of the institution. Specifically, we found that MCC New York staff failed to undertake required measures designed to make sure that, among other things, Epstein and other inmates were accounted for and safe, such as conducting inmate counts and 30-minute rounds, searching inmate cells, and ensuring adequate supervision of the Special Housing Unit (SHU) and the functionality of MCC New York’s security camera system. We further found that multiple BOP employees submitted false documents claiming that they had performed the required counts and rounds and that several MCC New York staff members lacked candor when questioned by the Office of the Inspector General (OIG) about their actions. Two MCC New York employees, Tova Noel and Michael Thomas, were charged criminally with falsifying BOP records relating to their conducting inmate counts and rounds. The U.S. Attorney’s Office for the Southern District of New York subsequently entered into deferred prosecution agreements with Noel and Thomas and the court dismissed all charges against them after Noel and Thomas successfully fulfilled the terms of their agreements. Prosecution was declined by the U.S. Attorney’s Office for the Southern District of New York for other MCC New York employees assigned to the SHU on August 9–10, 2019, who the OIG found also created, certified, and submitted false documentation regarding inmate counts and rounds on the day befo...
95 As detailed in Chapter 4 of this report, the SHU was a housing unit within MCC New York where inmates were securely separated from the general inmate population and kept locked in their cells for approximately 23 hours a day, to ensure their own safety as well as the safety of staff and other inmates. Access to the SHU was controlled by multiple locked doors. The primary entrance to the SHU (Main Exterior Entry Door) was opened remotely by a staff member in MCC New York’s centralized Control Center. Additionally, there was a second locked door at the main entrance (Main Interior Entry Door), which could be opened only with a key held by a limited number of Correctional Officers (CO) while on duty.55 Within the SHU, the entrance to each tier could be accessed only via a single locked door at the top or bottom of the staircase leading to the individual tier. Keys to open the locked tier doors were available only to a limited number of COs while on duty. Each tier had eight cells, each of which could house either one or two inmates. Each individual cell, which was made of cement and metal, could be accessed only through a single locked door, to which only a limited number of COs had keys while on duty. The SHU cell doors were made of solid metal with a small glass window and small locked slots that correctional staff used to handcuff inmates and provide food and toiletries to inmates. As a further security measure, during each shift a limited number of the COs had keys while on duty. BOP policy and practice require that all SHU inmates be locked in their cells overnight. The OIG found no evidence indicating that the door to Epstein’s cell or any other cell in the SHU tier in which Epstein was housed was unlocked on the evening of August 9–10, 2019, after SHU staff locked Epstein in his cell at approximately 8 p.m. SHU staff told the OIG that at approximately 8 p.m. on August 9, all SHU inmates were locked in their cells for the eve...
96 the L Tier during that timeframe other than the inmates who were locked in their assigned cells on that tier of the SHU. We also noted that the surveillance camera in the L Tier, as shown in the photograph in Figure 6.7, was in plain view of the inmates and therefore inmates would have been aware that any hallway movements, including into or out of Epstein’s cell, were being live streamed and could be monitored, even if, unbeknownst to them, the Digital Video Recorder (DVR) system was not recording the live stream at that time. As the OIG has noted in numerous prior reports regarding the BOP’s camera system, BOP staff and inmates are aware of where prison cameras are located and often engage in wrongdoing in locations where they know cameras are not located.56 Additionally, the OIG did not observe on the recorded video of the SHU common area that Noel and Thomas, who were seated at the desk at the SHU Officers’ Station immediately outside the L tier during that time period, at any time rose from their seats or approached the L Tier. We additionally found that Thomas’s and Noel’s reaction on the morning of August 10 upon finding Epstein hanging in his cell, as described to us by Thomas, Noel, the responding Lieutenant, and inmates, was consistent with their being unaware of any potential harm to Epstein prior to Thomas entering Epstein’s cell at about 6:30 a.m. on August 10. We further noted that Epstein had previously been placed on suicide watch and psychological observation due to the events of July 23, 2019; that numerous nooses made from prison bed sheets were found in his cell on the morning of August 10; and that he had signed a new Last Will and Testament on August 8, 2 days before he died. No weapons were recovered from Epstein’s cell after his death. Additionally, the inmates who were interviewed consistently reported that on the evening Epstein died the SHU staff did not systematically conduct the required rounds and counts...
97 management failures at multiple levels within the BOP.57 Similar to the Bulger report, the numerous and serious transgressions that occurred in this matter came to light largely because they involved a high-profile inmate. The fact that serious deficiencies occurred in connection with high-profile inmates like Epstein and Bulger is especially concerning given that the BOP would presumably take particular care in handling the custody and care of such inmates. Regrettably, the OIG has encountered similar issues on many other occasions. For example, the OIG has investigated numerous allegations related to the falsification of official BOP documentation concerning inmate counts and rounds, several of which have resulted in criminal prosecution. The OIG currently has two open investigations into allegations of falsified inmate count and round documentation, each involving an inmate death (by suicide and homicide) or escape from a BOP facility. This investigation and review also revealed the direct impact of insufficient staffing levels on inmate safety. Witnesses repeatedly told the OIG that counts, rounds, cell searches, and other methods of inmate accountability were not undertaken because correctional staff were working multiple shifts—including one staff member who worked 24-hours straight—and were tired and overwhelmed with other duties. As discussed in greater detail in our recommendations, the OIG has repeatedly found the need for BOP to address staffing shortages. Most recently, in March 2023, the OIG found that the coronavirus disease 2019 (COVID-19) pandemic exacerbated the effects of preexisting BOP medical and nonmedical staffing shortages, an issue the OIG has identified as a concern for the BOP since at least 2015.58 Further, the OIG has repeatedly found that BOP personnel have not consistently been attentive to the needs of inmates at risk for suicide. In this investigation, that inattention manifested in the failure of M...
98 The combination of negligence, misconduct, and outright job performance failures documented in this report all contributed to an environment in which arguably one of the most notorious inmates in BOP’s custody was provided with the opportunity to take his own life, resulting in significant questions being asked about the circumstances of his death, how it could have been allowed to have happen, and most importantly, depriving his numerous victims, many of whom were underage girls at the time of the alleged crimes, of their ability to seek justice through the criminal justice process. The fact that these failures have been recurring ones at the BOP does not excuse them and gives additional urgency to the need for Department of Justice (DOJ) and BOP leadership to address the chronic staffing, surveillance, security, and related problems plaguing the BOP. The OIG has completed its investigation and is providing this report to the BOP for appropriate action. Unless otherwise noted, the OIG applies the preponderance of the evidence standard in determining whether DOJ personnel have committed misconduct. The U.S. Merit Systems Protection Board applies this same standard when reviewing a federal agency’s decision to take adverse action against an employee based on such misconduct. See 5 U.S.C. § 7701(c)(1)(B) and 5 C.F.R. § 1201.56(b)(1)(ii). A. MCC New York Staff Failed to Ensure that Epstein Had a Cellmate on August 9 as Instructed by the Psychology Department on July 30 On July 30, 2019, the MCC New York Psychology Department sent an email to over 70 BOP staff members stating that Epstein “needs to be housed with an appropriate cellmate.” The Psychology Department’s directive that Epstein have an appropriate cellmate arose out of the events that occurred on July 23, 2019, when Epstein was found lying on the floor of his cell with a piece of orange cloth around his neck. Epstein’s cellmate at the time (Inmate 1) told MCC New York staff ...
99 resulted in Epstein being housed without a cellmate at the time of his death, which was contrary to the Psychology Department’s directive issued just 10 days earlier. BOP standards of conduct require that employees “obey the orders of their superiors at all times.”61 MCC New York Post Orders for the SHU require, among other things, that all SHU officers “maintain a log of pertinent information regarding inmate activity, detailing time, persons involved (if pertinent) and the event, which must be logged into TRUSCOPE.”62 Importantly, the SHU Post Orders clarify that they “are not intended to describe in detail all the officer’s responsibilities. Good judgment and common sense are expected in all situations not covered in these post orders.” On August 9, the Day Watch SHU Officer in Charge, the Evening Watch SHU Officer in Charge, and CO Tova Noel were each assigned to the MCC New York SHU as their permanent quarterly assigned post and served as the SHU Officer in Charge during their respective shifts.63 The OIG investigation found that each of these employees knew that Epstein was required to have a cellmate at all times per the Psychology Department’s directive. The OIG further found that on August 9 the Day Watch SHU Officer in Charge, the Evening Watch SHU Officer in Charge, and Noel each became aware at various times during their respective shifts that Epstein’s cellmate, Inmate 3, had been transferred from the institution with all of his belongings, a status known to all MCC New York staff members as meaning the inmate was being permanently transferred out of the institution. Specifically, the OIG investigation found that on the morning of August 9, the Day Watch SHU Officer in Charge and CO 1, who was also assigned to the SHU, reviewed the MCC New York daily call out list, a document that identifies all inmates who were leaving their housing units each day, which listed Inmate 3 as being scheduled to depart MCC New York with all...
100 The OIG investigation also found that during the next shift in the MCC New York SHU, both the Evening Watch SHU Officer in Charge and Noel became aware that Epstein was without a cellmate. The Evening Watch SHU Officer in Charge told the OIG that when he escorted Epstein back to his cell after Epstein’s telephone call, he saw that Inmate 3 was not there and then he, Noel, and the Material Handler discussed the need for Epstein to have a new cellmate. The Evening Watch SHU Officer in Charge also told the OIG that he notified an unspecified supervisor. However, other witnesses did not corroborate his account. Noel told the OIG that she was unaware both that Epstein needed to have a cellmate and that Inmate 3 had been removed from the institution. Noel also told the OIG that she went to Epstein’s cell at approximately 10 p.m.—a time of day when all inmates were secured in their cells—and may have plugged in Epstein’s medical device for him. The OIG did not credit Noel’s statements that she did not know that Epstein needed a cellmate or that Inmate 3 had been removed from the SHU based on contradictory witness statements (including her own) regarding SHU staff’s knowledge of Epstein’s cellmate requirement and Inmate 3’s transfer out of the SHU.66 The OIG investigation concluded that on August 9, 2019, the Day Watch SHU Officer in Charge, the Evening Watch SHU Officer in Charge, and Noel failed to notify a supervisor as required after Epstein’s cellmate was permanently removed from the MCC New York SHU, which constituted a violation of BOP standards of conduct. Additionally, their inaction violated MCC New York SHU Post Orders because none of these individuals documented the fact the Epstein needed a new cellmate as required. Finally, all of these officers failed to exercise good judgment and common sense, as required by the SHU Post Orders, by not immediately undertaking steps through their chain-of-command to ensure that a high-profi...
101 shifts, and the Captain had oversight over all of the Lieutenants.68 The OIG found that the failure of these individuals to adequately supervise SHU staff and ensure that a high-profile inmate who had recently been on suicide watch and psychological observation had an appropriate cellmate constituted a job performance failure. 3. Failure to Have a Contingency Plan for Assigning Epstein a Cellmate Additionally, the OIG found that the Warden’s failure to have a back-up cellmate assignment for Epstein constituted poor judgment. The Evening Watch SHU Officer in Charge told the OIG that although he knew that Epstein needed to be assigned another cellmate, SHU staff could not just put anyone in the cell with Epstein. The Warden confirmed this in his OIG interview, when he explained that he and BOP executive leadership selected Inmate 3 as Epstein’s cellmate following the events of July 23, 2019. The Warden told the OIG that no inmates were pre-vetted to serve as Epstein’s cellmate if Inmate 3 left MCC New York. 69 The Northeast Regional Director, the Warden, and the Captain all told the OIG that if Inmate 3 had been removed as Epstein’s cellmate, they would have had to review a new list of potential cellmate candidates to ensure that Epstein was housed with an appropriate inmate. This selection process, which involved multiple steps undertaken by high-level BOP management, would be difficult to accomplish in a short period of time and ultimately may have impeded SHU officers’ ability to house Epstein with a cellmate on August 9, 2019. 4. Lack of Candor BOP policy requires that “[d]uring the course of an official investigation, employees are to cooperate fully by providing all pertinent information they may have. Full cooperation requires truthfully responding to questions.”70 As discussed above, the Day Watch SHU Officer in Charge and the Evening Watch SHU Officer in Charge told the OIG that they notified supervisory personnel regardin...
102 email identifying the cellmate requirement; and the statements of multiple witnesses who told the OIG that Epstein’s cellmate requirement was widely disseminated verbally by MCC New York leadership. B. MCC New York Staff Failed to Conduct Mandatory Rounds and Inmate Counts Resulting in Epstein Being Unobserved for Hours Before His Death The OIG’s investigation and review revealed that on August 9 and 10, 2019, MCC New York SHU staff did not conduct the mandatory rounds and inmate counts during their shift in the SHU. The failure to undertake these required measures to account for inmate whereabouts and wellbeing—and the supervisors’ failure to properly supervise the SHU staff, as discussed further below—resulted in Epstein being unobserved for hours before his death, which compounded the failure of MCC New York staff to ensure that Epstein had an appropriate cellmate. 1. Failure to Conduct Rounds and Inmate Counts in the SHU Federal regulations require that employees “use official time in an honest effort to perform official duties.”71 Additionally, BOP standards of conduct required that employees “[c]onduct themselves in a manner that fosters respect for the Bureau of Prisons, the Department of Justice, and the U.S. Government.”72 Because “[i]nattention to duty in a correctional environment can result in escapes, assaults, and other incidents,” BOP standards of conduct also require employees “to remain fully alert and attentive during duty hours.” BOP policy also requires “[c]ontinuous inmate accountability,” which is accomplished through rounds and inmate counts.73 Among other things, rounds and inmate counts enable staff to observe inmates and ensure that they are safe and secure in their cells and are in good health. BOP policy and MCC New York SHU Post Orders set out the requirements for these inmate accountability measures, specifying that correctional staff must conduct rounds on an irregular schedule at least twice each ho...
103 on the evening of August 9 and the morning of August 10. Noel told the OIG that she conducted the 10 p.m. count on August 9. The OIG did not credit her statement based on: (1) its review of the SHU security camera video, which reflects Noel walking up and down the stairs leading to some, but not all, of the tiers several minutes after the SHU inmate count had been called into the Control Center; (2) the 10 p.m. count slip, which erroneously included the SHU Inmate 4, who had been internally transferred to Receiving and Delivery; (3) other BOP records; and (4) the Material Handler’s statement to the OIG that no one conducted the 10 p.m. count because everyone was tired. Instead of performing the required duties to account for inmate whereabouts and wellbeing, the OIG found that officers assigned to the SHU on August 9 and 10, including the Material Handler, Noel, and Thomas primarily remained seated in the SHU Officers’ Station—sometimes without moving for a period of time, suggesting that they were asleep—and conducted a variety of Internet searches on MCC New York computers. Thomas also admitted to the OIG that he “dozed off” for periods of time during his shift. The OIG’s analysis of the SHU security camera video revealed that after approximately 10:40 p.m., no CO entered Epstein’s tier in the SHU until just before 6:30 a.m. when Noel and Thomas began to serve breakfast to the inmates. The OIG investigation and review concluded that the Evening Watch SHU Officer in Charge, the Material Handler, Noel, and Thomas failed to conduct the mandatory rounds and inmate counts during their respective shifts in the MCC New York SHU on August 9 and 10, 2019, and that their actions constituted violations of 5 C.F.R. §§ 2635.101(b)(5) and 2635.705(a), BOP Program Statements 3420.11 and 5500.14, and MCC New York SHU Post Orders. 2. False Statements and Lack of Candor The OIG’s investigation and review found that on August 9 and 10, 2019, the Ev...
104 inmate was accounted for.76 Only after all the count slips have been collected from each housing unit, and the numbers on the count slips had been matched to the institution’s overall inmate count sheet, could the institutional count be deemed “cleared” or completed. The Evening Watch SHU Officer in Charge, the Material Handler, Noel, and Thomas each prepared and/or signed a false count slip to create the impression that they had fulfilled their inmate accountability responsibilities when, in fact, they had not.77 These individuals admitted to the OIG that instead of performing their assigned duties, they pre-filled the count slips with the number of inmates they believed were in the SHU based on what officers from the previous shift had told them and signed off on the documents knowing that they falsely attested to having completed the counts. Additionally, Noel admitted to the OIG that she had prefilled the official MCC New York forms documenting the times of the 30-minute rounds, often referred to as round sheets, and falsely attested to having completed the rounds.78 Noel and Thomas were indicted by a grand jury for their false certifications of having conducted counts and rounds. Subsequently, each entered into a deferred prosecution agreement with the U.S. Attorney’s Office for the Southern District of New York. The U.S. Attorney’s Office of the Southern District of New York declined prosecution for the Evening Watch SHU Officer in Charge and the Material Handler. The OIG investigation has found that the Evening Watch SHU Officer in Charge, the Material Handler, Noel, and Thomas knowingly and willingly falsified BOP records in violation of federal law by attesting that they had completed the mandatory rounds and inmate counts on the evening of August 9, 2019, and morning of August 10, 2019. Additionally, as noted above, BOP policy requires employees to cooperate fully with an official investigation and truthfully respond to qu...
105 minimum elapsed time of on ‘days off’ will be fifty-six (56) hours, except when the employee requests the change.”79 The Material Handler told the OIG that on August 9 he reported for a voluntary overtime shift from 12 a.m. to 8 a.m. and then worked his regular 8 a.m. to 4 p.m. shift in the warehouse. At some point during the day shift, the Day Watch Operations Lieutenant, a higher ranking official, called and asked the Material Handler if he could work overtime in the SHU and he agreed. The Material Handler told the OIG that he felt pressured to work the third shift, which resulted in him working 24 hours straight, from 12 a.m. on August 9 through 12 a.m. on August 10. As discussed previously, the Material Handler admitted to the OIG that on the evening of August 9, during his third shift which he worked in the SHU, he did not conduct the mandatory inmate counts and rounds because he was too tired. The OIG investigation and review concluded that the Day Watch Operations Lieutenant exercised poor judgment when he requested that the Material Handler work a third consecutive shift. As the Day Watch Operations Lieutenant, he had access to the staff roster and schedule and therefore he should have known that the Material Handler had already worked 16 straight hours. Additionally, the Day Watch Operations Lieutenant’s action was inconsistent with the collective bargaining agreement and did not reflect sound correctional judgment, as it would have been extremely difficult for the Material Handler to have effectively performed his duties during his third shift. 4. Clearing the 10 p.m. Institutional Count Knowing that It Was Inaccurate The OIG’s investigation and review determined that on August 9, 2019, MCC New York staff cleared the 10 p.m. institutional count knowing that the inmate counts from two housing units were inaccurate. BOP policy and MCC New York SHU Post Orders require that COs conducting an institutional count relay the coun...
106 count. Senior Officer Specialist 6 explained that the action he took was known as “ghost counting,” something he said he would not have done without authorization from the Operations Lieutenant or someone of a higher rank than himself. The Morning Watch Operations Lieutenant denied having authorized a “ghost count” and we found no evidence to corroborate Senior Officer Specialist 6’s claim that the Morning Watch Operations Lieutenant knew of and approved the false count. The OIG found that Senior Officer Specialist 6 modified the count slips received from the SHU and Receiving and Discharge, failed to request a recount of the SHU inmates, and cleared the 10 p.m. institutional count knowing that it was inaccurate in violation of BOP policy and MCC New York SHU Post Orders. 5. Failure to Adequately Supervise SHU Staff and Conduct Lieutenant Rounds The OIG also found that MCC New York supervisory personnel failed to effectively perform their duties, which contributed to the fact that Epstein was unobserved for many hours before his death. As discussed above, federal regulations require that MCC New York supervisory personnel “put forth honest effort in the performance of their duties,” which includes appropriate supervision of SHU personnel.81 Additionally, BOP policy requires that a Lieutenant visit the SHU during each shift to ensure that all procedures are being followed.82 The OIG’s investigation revealed that the Evening Watch Operations Lieutenant and the Morning Watch Operations Lieutenant had oversight of the SHU during their respective shifts.83 The Evening Watch Operations Lieutenant told the OIG that on August 9, 2019, he did not supervise the 4 p.m. count or conduct any rounds in the SHU. He acknowledged that he signed some of the pages of the 4 p.m. count, but he did not sign all of the pages as he should have. Beginning at 10 p.m. on August 9, the Morning Watch Operations Lieutenant was the sole supervisor overseeing th...
107 is inconsistent with the statements of many other supervisors and BOP Lieutenant training, all of which emphasized the need for Lieutenants to walk down all of the SHU tiers during a round. During their interviews with the OIG, the Northeast Regional Director, the Warden, Associate Warden 1, and the Captain clarified that they expected a Lieutenant conducting a round in the SHU to check in with the officers, walk down each of the tiers in the SHU, speak with inmates, and address inmate concerns. They explained that the Lieutenants did not act responsibly if they did not walk down each of the tiers to check on the inmates in the SHU. As the Acting Evening Watch Activities Lieutenant explained, unlike inmates in general population, SHU inmates cannot approach a supervisor because they are confined within a cell. Further, the BOP Lieutenant training, which the Morning Watch Operations Lieutenant attended in 2011, taught that Operations Lieutenants were required to visit the SHU at least once during each shift and that “[t]his visit will be substantially more than just entering the unit, signing the log book, and talking with staff.” Instead, Operations Lieutenants were trained to, among other things, walk through each range (or tier), inspect logs and reports, observe activities, and periodically observe counts within the SHU. The OIG found that the failure of the Evening Watch Operations Lieutenant and the Morning Watch Operations Lieutenant to adequately supervise SHU staff, and of the Morning Watch Operations Lieutenant to adequately conduct a Lieutenant round in the SHU, which contributed to the SHU staff’s failure to conduct mandatory rounds and counts, constituted a job performance failure. C. MCC New York Staff Allowed Epstein to Place an Unmonitored Telephone Call on August 9 The OIG’s investigation and review revealed that on the night before his death, Epstein placed an unrecorded, unmonitored telephone call using a non-Inma...
108 investigation established both that Epstein’s mother was deceased at the time he asked to telephone her and that Epstein had been assigned the necessary documentation that would have allowed him to place calls through the Inmate Telephone System, although he did not take the necessary steps to complete the setup process that would have given him the ability to place calls through that system. The Captain told the OIG that when the Unit Manager was escorting Epstein from his attorney visit back to the SHU and Epstein’s requested call was discussed, he told the Unit Manager that Epstein’s telephone call had to be monitored and logged. The Unit Manager told the OIG that he escorted Epstein from his attorney visit to the shower area of the SHU, where he connected a telephone into an unrecorded legal line and dialed the phone number provided by Epstein. The Unit Manager said that when a male answered the call, he handed the telephone to Epstein, and then left MCC New York for the day because his shift had ended. Before leaving the SHU, the Unit Manager said he told the Evening Watch SHU Officer in Charge, the Material Handler, and Noel, who were at the SHU Officers’ Station, to make sure Epstein got his 15 minutes on the telephone, but he did not instruct them to monitor the telephone call. The Unit Manager admitted that he did not verify the recipient of the telephone call, and that neither he nor anyone monitored or logged the telephone call as required. The OIG found that the Unit Manager violated BOP policy by allowing Epstein to make an unrecorded and unmonitored telephone call, and by failing to verify the telephone call recipient, monitor, and log the call. We further found that the Unit Manager exercised poor judgment when he left MCC New York while Epstein was still on the telephone call that the Unit Manager had arranged and failed to instruct the Evening Watch SHU Officer in Charge, the Material Handler, or Noel to monitor the ...
109 TRUSCOPE, but that it was primarily the SHU Officer in Charge’s responsibility to do so. The Evening Watch SHU Officer in Charge told the OIG that he and other staff members did not conduct any cell searches during his shift in the SHU on August 9. Additionally, the OIG determined that there was an excessive amount of bed linen within Epstein’s cell. The Captain reviewed photographs of Epstein’s cell and told the OIG that the excessive linens were a security issue because they could give inmates materials to fashion an improvised noose or use as escape paraphernalia. The OIG found that on August 9, 2019, the Day Watch SHU Officer in Charge either failed to conduct the required cell searches or failed to document the cell searches that he conducted in the SHU, and that the Evening Watch SHU Officer in Charge failed to ensure that MCC New York staff assigned to the SHU conducted cell searches and himself failed to log cell searches in violation of BOP policy and MCC New York SHU Post Orders. Additionally, the OIG found that it was a performance failure for the Day Watch SHU Officer in Charge, the Evening Watch SHU Officer in Charge, and Noel, who served as the SHU Officer in Charge during their respective shifts on August 9 and 10, 2019, to have permitted Epstein to have an excessive amount of linens in his cell. E. MCC New York Staff Failed to Ensure that the Institution’s Security Camera System was Fully Functional Resulting in Limited Recorded Video Evidence This investigation and review revealed longstanding deficiencies with MCC New York’s security camera system. These deficiencies resulted in nearly all of the cameras in and around the SHU where Epstein was being housed to not record video starting in late July 2019 and continuing through the date of Epstein’s death on August 10, 2019. According to forensic analysis conducted by the FBI after Epstein’s death, on July 29, 2019, a disk failure in MCC New York’s DVR 2 system caus...
110 MCC New York’s failure to ensure that its security camera system was fully functional and make timely repairs is consistent with the OIG’s previous observations regarding weaknesses in the BOP’s overall system of security cameras. Dating back to at least 2013, the OIG has repeatedly observed inadequacies in the BOP’s overall system of security cameras, including inoperable cameras, an insufficient number of cameras, poor video quality, and inadequate video storage. In a 2016 report on the BOP’s contraband interdiction efforts, the OIG identified specific deficiencies with the camera system, and recommended that the BOP evaluate the system to determine needed upgrades.88 In response to the 2016 recommendation, the BOP assessed the camera systems at each institution over the next several years and determined that 45 of its 122 institutions, including MCC New York, required camera system upgrades. The BOP worked to upgrade the systems at those 45 institutions between 2019 and 2021. In June 2021, the BOP reported that it had updated all cameras at the 45 institutions with the latest software and equipment, and that it had installed additional cameras to bolster surveillance. However, as reported in an October 2021 Management Advisory Memorandum issued to the BOP, the OIG analyzed the reported upgrades at the 45 institutions and found that the BOP had addressed some but not all of the deficiencies described in the 2016 OIG report. In its 2021 Management Advisory Memorandum, the OIG recommended that the BOP develop a comprehensive strategic plan for transitioning to a fully digital security camera system. The BOP has provided the OIG with a strategic plan that includes estimated cost projections and timelines for addressing the camera system concerns and completing the system upgrades.89 As of 2023, the OIG’s 2021 recommendation remains open. The BOP’s failure to address the issue of functional security camera systems across the agency...
111 policy does not, however, describe how long the cellmate requirement should last or if any staff must approve the removal of the cellmate requirement. The Suicide Prevention Program Policy Statement 5324.08 does not describe any process or procedure that requires cellmate assignments for inmates coming off of suicide watch. The Warden stated there was no BOP policy mandating that an inmate coming off of suicide watch have a cellmate, but that doing so was “sound correctional judgment.” The OIG’s investigation and review revealed that there were knowledge gaps among MCC New York staff regarding Epstein’s cellmate requirement, indicating that improved communication with institutional staff would be beneficial. The OIG therefore recommends that the BOP implement a requirement that all inmates coming off of suicide watch or psychological observation to be assigned cellmates with criteria for exceptions based on the particular individual or security considerations, provide guidance for determining when a cellmate is no longer required, and implement a process for approving, documenting, and communicating to institutional staff the assignment and removal of cellmates for these inmates. 2. The BOP should establish procedures to ensure inmates at high risk for suicide and for whom a cellmate is recommended will continue to have a cellmate until the recommendation is changed or rescinded, including establishing a contingency plan for cellmate re-assignment, with criteria for exceptions based on the particular individual or security considerations. The OIG’s investigation and review found that there was no contingency plan in place to assign Epstein a new cellmate when his then-cellmate was transferred out of MCC New York. Although the failure to assign a new cellmate was due, in part, to SHU staff failing to make required notifications and supervisory staff failing to adequate supervise SHU staff, the gap in cellmate assignment was also due ...
112 MCC New York Procedural Memorandum for Psychological Observation states that inmates on psychological observation will be continuously monitored by either an inmate companion or a staff member. A review of the Suicide Watch Chronological Logs for July 23, 2019, revealed Epstein was allowed to leave the suicide watch room to visit with his attorneys for more than 6 hours. According to the Psychological Reconstruction conducted by the Assistant Director of the Reentry Services Division, during Epstein’s psychological observation on July 24 through July 30, 2019, Epstein was also allowed to visit with his attorneys between 8–11 hours each day without direct observation. Although the MCC New York supplemental policy described an approval process for social and legal visits while an inmate is on suicide watch or psychological observation, the OIG found no evidence that Epstein’s legal visits were approved by the Captain or an Associate Warden. Additionally, the BOP Suicide Prevention Program Policy Statement 5324.08 does not describe any process or procedures that allows an inmate to have legal or social visits while on suicide watch or psychological observation. The OIG therefore recommends that the BOP evaluate its current process for such visits to be approved and documented. 4. The BOP should evaluate its methods of accounting for inmate whereabouts and wellbeing and make changes as may be appropriate to improve those methods through policy, training, or other measures. The OIG’s investigation and review revealed many inmate accountability deficiencies. Most fundamentally, MCC New York staff assigned to the SHU on August 9 and 10, 2019, did not conduct many of the required rounds and inmate counts. Additionally, there was lacking or delayed documentation regarding inmates, including cell assignments and internal inmate transfers. Internal reports, such as the daily call out list and the Lieutenant log, are either not retained or s...
113 6. The BOP should continue to develop and implement plans to address staffing shortages at its prisons. Since at least 2015, the OIG has repeatedly found the need for BOP to address staffing shortages, including medical staffing shortages.90 This investigation and review revealed the direct impact of staffing deficiencies on inmate safety. For example, the Material Handler worked three consecutive shifts—24 hours straight— on August 9, 2019, which was certainly a contributory cause to the lack of adequate means of accounting for inmate location and wellbeing in the SHU. The Material Handler told the OIG that no one did the 10 p.m. SHU inmate count because they were tired. Additionally, the OIG’s investigation and review found that in connection with MCC New York’s upgrade of its security camera system, the BOP’s Northeast Regional Office arranged for technicians from other BOP institutions to perform temporary duty (TDY) assignments to MCC New York to perform necessary mechanical, electrical, plumbing, and wiring work. Yet, during the course of the TDY rotations, work was not consistently conducted on the camera upgrade because sometimes TDY staff were used to cover shortages at MCC New York’s custody posts. Without adequate staffing, the BOP cannot fulfill its mandate to ensure safe and secure correctional facilities. The OIG therefore recommends that the BOP continue to develop and implement plans to address staffing shortages at its institutions. 7. The BOP should evaluate its cell search procedures and make changes as may be appropriate to improve those procedures through policy, training, or other measures. The OIG’s investigation and review found that there was an excessive amount of linens in Epstein’s cell at the time of his death. BOP policy and MCC New York SHU Post Orders require that SHU cells be searched, but they do not specifically address the issue of excessive bed linens, which the Captain told the OIG present a...
114 8. The BOP should enhance existing policies regarding institutional security camera systems to ensure they specifically state that such systems must have the capacity to record video and that BOP institutions must conduct regular security camera system functionality checks. As discussed in the Conclusions section of this chapter, the OIG found that, even though the highest levels of leadership knew of the MCC New York security camera system’s recurring deficiencies, prior to Epstein’s death, no one was tasked with the responsibility of checking the security camera system on a routine basis to ensure that the system was functional. As a result, when on July 29, 2019, video from approximately half of the institution’s security cameras was no longer being recorded, the problem went undetected for 11 days. The OIG also found that there are no BOP policies that specifically state that security camera systems must have the capacity to record or that institutional staff must perform periodic checks to ensure the camera system is fully functional. Cameras that are failing to provide good quality or any live video streams put the safety of BOP staff members and inmates at risk, and the lack of video recordings can potentially hinder investigations of wrongdoing by staff and inmates. The OIG therefore recommends that the BOP enhance existing policies and protocols so they specifically state that all institutional security camera systems must have the capacity to record, and that specified staff at each institution must conduct periodic checks of the security camera system to determine its operational status and take corrective action as soon as possible when the system is found to be inoperable. Such routine checks would help ensure that camera system malfunctions are detected and corrective actions are initiated in a timely manner.
115 Appendix A: The BOP’s Response to the Draft Report Office of the Director U. S. Department of Justice Federal Bureau of Prisons Central Office Washington, DC 20534 June 22, 2023 MEMORANDUM FOR SARAH E. LAKE FROM: SUBJECT: ASSISTANT INSPECTOR GENERAL INVESTIGATIONS DIVISION Colette S. Peters, Director Response to the Office oflnspector General's (OIG) Draft Report: Investigation and Review of the Federal Bureau of Prisons' Custody, Care, and Supervision of Jeffrey Epstein at the Metropolitan Correctional Center in New York, New York The Bureau of Prisons (BOP) appreciates the opp011unity to formally respond to the Office of the Inspector General's (OIG) above-referenced draft report. BOP values OIG's careful review of the facts and circumstances surrounding the death of Jeffrey Epstein and concurs with the recommendations resulting from this engagement. The lessons learned during the course of this engagement will be applied to the broader BOP correctional landscape. The facts and circumstances related to those few BOP employees at MCC New York in this report reflect a failure to follow BOP's longstanding policies, regulations, and/or laws. While this misconduct described in this report is troubling, those who took part in it represent a very small percentage of the approximately 35,000 employees across more than 120 institutions who continue to strive for correctional excellence every day. In the Report, OIG makes recommendations to enhance BOP policies and practices and improve accountability. In response to this and previous OIG and Government Accountability Office (GAO) engagements, BOP has already begun to evaluate nationwide trends and strengthen employee accountability.
116 OIG Official Draft Report: BOP's Care, Custody, and Supervision of Jeffrey Epstein at MCC New York, New York June 22, 2023 Page 2 of3 In April of this year, BO P's leadership announced its new mission as "corrections professionals who foster a humane and secure environment and ensure public safety by preparing individuals for successful reentry into our communities." BOP's new core values include accountability, integrity, respect, compassion, and correctional excellence. Of note, our core value of accountability requires BOP employees to be responsible and transparent to the public, ourselves, and to those in our care and custody by the standards we establish, the actions we take, and the duties we perform. As reflected in our mission and core values, BOP is committed to providing a safe environment for both employees and adults in our custody. Recommendation One: The BOP should implement a process for assigning a cellmate following suicide watch or psychological observation, with criteria for exceptions based on the particular individual or security considerations. BOP's Response: The BOP recognizes the impo11ance of careful monitoring of adults in custody who face mental health challenges and therefore concurs with this recommendation. Our practice is to carefully consider both the well-being and safety of the individual involved and overarching safety and security concerns. In the years since Mr. Epstein's death, the BOP has updated its process related to suicide watch and psychological observation. Under BOP's revised process, upon removal from suicide watch or psychological observation, psychologists make individualized care recommendations about clinical follow-up and other custodial concerns, including housing and cellmates. Mental health, custody, and unit team employees work collaboratively to ensure that each individual removed from suicide watch is housed appropriately. Recommendation Two: The BOP should establish pr...
117 OIG Official Draft Report: BOP's Care, Custody, and Supervision of Jeffrey Epstein at MCC New York, New York June 22, 2023 Page 3 of3 BOP's Response: The BOP concurs with this recommendation. Recommendation Four: The BOP should evaluate its methods of accounting for inmate whereabouts and wellbeing and make changes as may be appropriate to improve those methods through policy, training, or other measures. BOP's Response: The BOP concurs with this recommendation. Recommendation Five: BOP policy should clarify what is required of a lieutenant when conducting a round. BOP's Response: The BOP concurs with this recommendation. Recommendation Six: The BOP should continue to develop and implement plans to address staffing shortages at its prisons. BOP's Response: The BOP concurs with this recommendation. Hiring and retaining qualified personnel is a key priority and BOP has developed and implemented a multi-pronged approach that involves enhanced recruitment efforts and appropriate incentives. While the issues raised in the OIG's report were the result of employees failing to adhere to their duties, as opposed to a staffing shortage, the BOP welcomes the opportunity to continue the significant work that has already been undertaken and that is ongoing regarding staffing. Recommendation Seven: The BOP should evaluate its cell search procedures and make changes as may be appropriate to improve those procedures through policy, training, or other measures. BOP's Response: The BOP concurs with this recommendation. Recommendation Eight: The BOP should enhance existing policies regarding institutional security camera systems to ensure they specifically state that such systems must have the capacity to record video and that BOP institutions must conduct regular security camera system functionality checks. BOP's Response: The BOP concurs with this recommendation. The BOP appreciates OIG's careful attention to this engagement, and its willingn...
118 Appendix B: OIG Analysis of the BOP’s Response The Office of the Inspector General (OIG) provided a draft of this report to the Federal Bureau of Prisons (BOP), and the BOP’s response is incorporated as Appendix A. The BOP indicated in its response that it agreed with all eight recommendations. The following provides the OIG’s analysis of the BOP’s response and a summary of the actions necessary to close the recommendations. The OIG requests that the BOP provide an update on the status of its response to the recommendations within 90 days of the issuance of this report. Recommendation 1: The BOP should implement a process for assigning a cellmate following suicide watch or psychological observation, with criteria for exceptions based on the particular individual or security considerations. Status: Resolved. BOP Response: The BOP reported the following: The BOP recognizes the importance of careful monitoring of adults in custody who face mental health challenges and therefore concurs with this recommendation. Our practice is to carefully consider both the well-being and safety of the individual involved and overarching safety and security concerns. In the years since Mr. Epstein’s death, the BOP has updated its process related to suicide watch and psychological observation. Under BOP’s revised process, upon removal from suicide watch or psychological observation, psychologists make individualized care recommendations about clinical follow-up and other custodial concerns, including housing and cellmates. Mental health, custody, and unit team employees work collaboratively to ensure that each individual removed from suicide watch is housed appropriately. OIG Analysis: The BOP’s response is responsive to this recommendation. The OIG will consider whether to close this recommendation after the BOP (1) provides for the OIG’s review a proposed process for assigning a cellmate following suicide watch or psychological observat...
119 individualized approach to the care and custody of adults in custody. Upon removal from suicide watch or psychological observation, individualized care recommendations are made by psychologists, custody, and unit team for each individual. BOP thoroughly evaluates each celling assignment on an individual basis for persons deemed to be at moderate to high risk for suicide. OIG Analysis: The BOP’s response is not fully responsive to this recommendation. Recommendation 1 focuses on the process for assigning a cellmate following suicide watch and psychological observation. Recommendation 2, on the other hand, focuses on procedures to ensure that inmates at high risk for suicide and for whom a cellmate is recommended continue to have a cellmate until the recommendation is changed or rescinded. Our investigation and review determined that BOP employees did not take steps to ensure that Jeffrey Epstein continuously had a cellmate in response to Psychology Department personnel having determined that he needed to have an appropriate cellmate, and absent any indication that security or other considerations relating to Epstein warranted his not having a cellmate. The OIG will consider whether to close this recommendation after the BOP (1) develops the recommended procedures; (2) provides the procedures to the OIG; and (3) implements the procedures. Recommendation 3: The BOP should evaluate its current process for obtaining and documenting approval for social or legal visits while an inmate is on suicide watch or psychological observation, which allows for institution-specific variations in the process, and provide guidance on standard components that each institution should include in its process to mitigate security issues that can arise when an inmate is on suicide watch or psychological observation. Status: Resolved. BOP Response: The BOP reported the following: The BOP concurs with this recommendation. OIG Analysis: The BOP concurr...
120 OIG Analysis: The BOP concurred with this recommendation but did not provide any additional information. The OIG will consider whether to close this recommendation after the BOP (1) evaluates its methods of accounting for inmate whereabouts and wellbeing; (2) makes any appropriate changes to improve those methods through policy, training, or other measures; and (3) provides documentation of evaluation and any appropriate changes to the OIG. Recommendation 5: BOP policy should clarify what is required of a Lieutenant when conducting a round. Status: Resolved. BOP Response: The BOP reported the following: The BOP concurs with this recommendation. OIG Analysis: The BOP concurred with this recommendation but did not provide any additional information. The OIG will consider whether to close this recommendation after the BOP (1) updates its policy to clarify what is required of a Lieutenant when conducting a round; (2) communicates the policy update to all relevant BOP employees; and (3) provides documentation of the policy update and communication to the OIG. Recommendation 6: The BOP should continue to develop and implement plans to address staffing shortages at its prisons. Status: Resolved. BOP Response: The BOP reported the following: The BOP concurs with this recommendation. Hiring and retaining qualified personnel is a key priority and BOP has developed and implemented a multi-pronged approach that involves enhanced recruitment efforts and appropriate incentives. While the issues raised in the OIG’s report were the result of employees failing to adhere to their duties, as opposed to a staffing shortage, the BOP welcomes the opportunity to continue the significant work that has already been undertaken and that is ongoing regarding staffing. OIG Analysis: The BOP’s response is responsive to the recommendation. The OIG will consider whether to close this recommendation after the BOP (1) develops and implements plans to a...
121 OIG Analysis: The BOP concurred with this recommendation but did not provide any additional information. The OIG will consider whether to close this recommendation after the BOP (1) evaluates its cell search procedures; (2) makes any appropriate changes to those procedures through policy, training, or other measures; and (3) provides documentation of evaluation and any appropriate changes to the OIG. Recommendation 8: The BOP should enhance existing policies regarding institutional security camera systems to ensure they specifically state that such systems must have the capacity to record video and that BOP institutions must conduct regular security camera system functionality checks. Status: Resolved. BOP Response: The BOP reported the following: The BOP concurs with this recommendation. OIG Analysis: The BOP concurred with this recommendation but did not provide any additional information. The OIG will consider whether to close this recommendation after the BOP (1) enhances existing policies regarding institutional camera systems to include the recommended language update; (2) communicates the policy update to all relevant BOP employees; and (3) provides documentation of the policy update and communication to the OIG.
Size: 9 x 60 pixels
Small redaction (~1 chars)
Size: 20 x 17 pixels
Small redaction (~2 chars)
Size: 34 x 15 pixels
Small redaction (~3 chars)
Size: 14 x 20 pixels
Small redaction (~1 chars)
Size: 9 x 31 pixels
Small redaction (~1 chars)
Size: 31 x 33 pixels
Surrounding text: Camer
Small redaction (~3 chars)

Page 1
property
1397 x 486
Objects: Architecture, Building, Office Building, City, Urban, Pillar
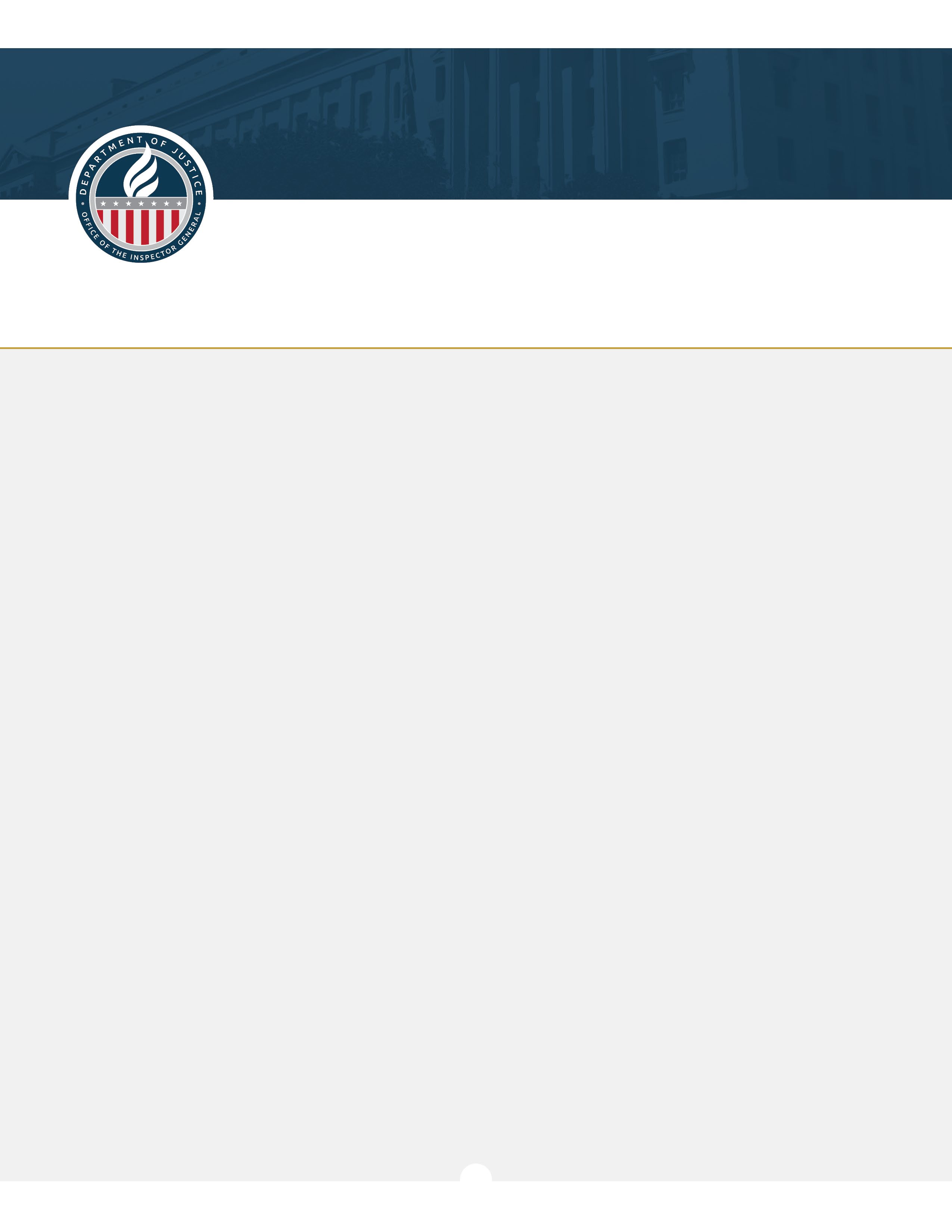
Page 2
photo
2550 x 3300
Text: DEPARTMENT OFFICE OF THE INSPECTOR OF JUSTICE GENERAL

Page 2
photo
357 x 357
Objects: Logo, Emblem, Symbol | Text: JUSTICE | OF | OFFICE | GENERAL | OF

Page 31
photo
1317 x 617
Objects: Door, Indoors | Text: SPECIAL-HOUSING | UNIT | 9 SOUTH | North | Main Interior

Page 32
photo
942 x 753
Objects: Chair, Furniture, Indoors | Text: South | Elevator Bay | Main Entry Door | (not pictured)

Page 33
diagram
2100 x 1052
Objects: Diagram, Scoreboard, Clapperboard | Text: Lower Tiers | Upper Tiers | L Tier | M Tier | J T

Page 34
diagram
1280 x 720
Objects: Diagram | Text: JTier | L Tier | к Tier | M Tier | 9th Floor

Page 35
property
1194 x 694
Objects: Architecture, Building, House, Housing, Staircase, Handrail, Bench, Furniture, Indoors | Te

Page 42
property
1255 x 638
Objects: Architecture, Building, Indoors, Corridor | Text: 219 | Epstein's | Cell

Page 43
photo
1210 x 438
Objects: Door, Indoors, Person | Text: L Tier | Entry Door | CRIME SCENE DO NOT CROSS | CENE | DO
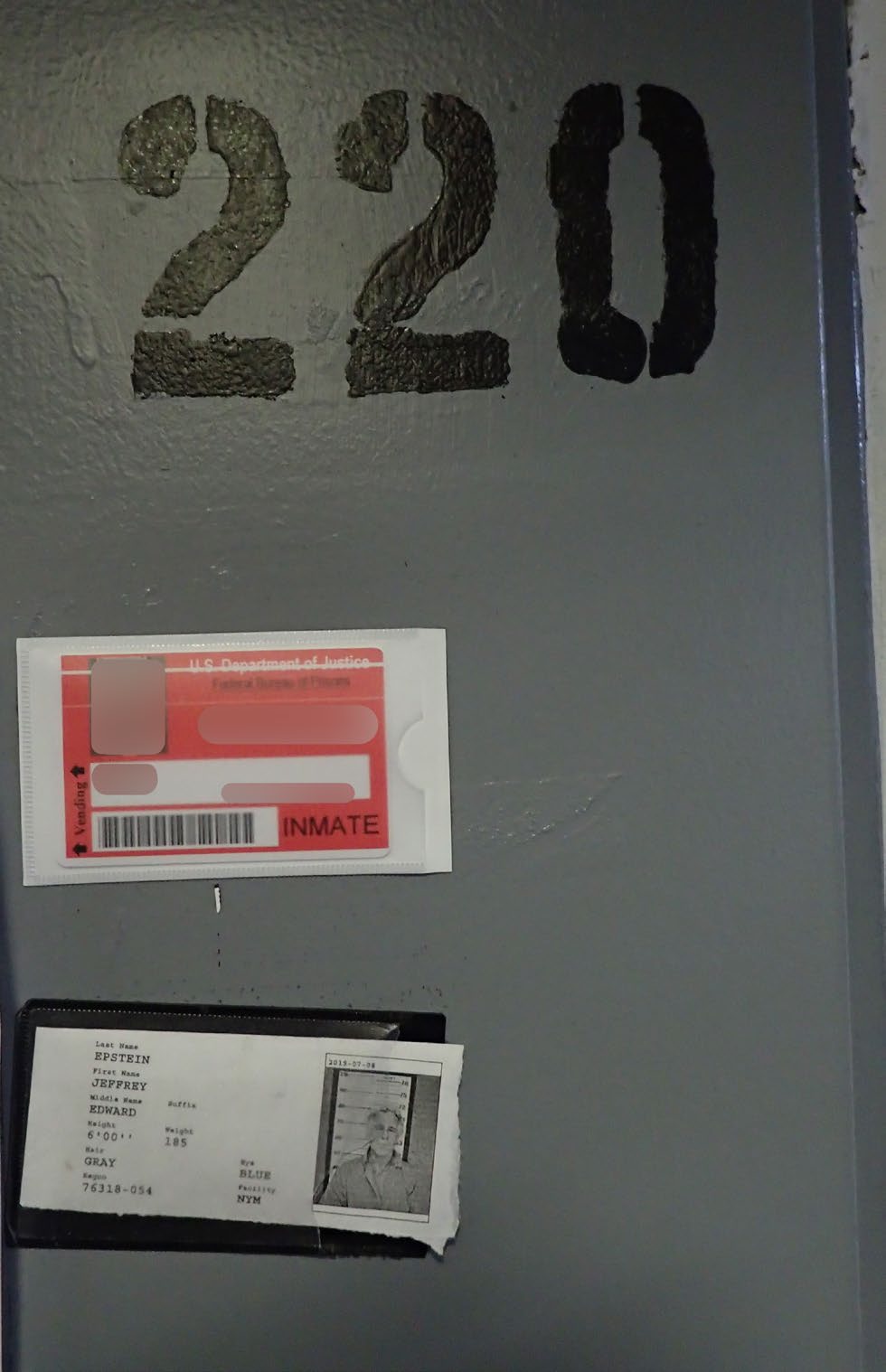
Page 44
document
980 x 1518
Objects: Text, Number, Symbol, Business Card, Paper, Person | Text: 220 | INMATE | Vending | EPSTEIN

Page 45
photo
996 x 645
Objects: Indoors

Page 46
photo
1253 x 432
Objects: Furniture, Indoors

Page 47
photo
1076 x 701
Objects: Furniture, Table | Text: TIER | Z06 | Epstein's Cell Door | Officers' | Station

Page 48
photo
1258 x 701
Objects: Prison | Text: Officers' | Station | Officers' | Epstein's | Station

Page 72
document
1909 x 640
Objects: Text, Document | Text: Metropolitan Correctional Center | Metropolitan Correctional Center

Page 75
document
831 x 640
Objects: Book, Publication, Advertisement, Text, Poster, Paper | Text: MANADATORY ROUNDS MUST | BE C

Page 78
property
406 x 541
Objects: Furniture, Architecture, Building, Hostel, Housing, Bed, Indoors

Page 81
diagram
571 x 574
Objects: Chart, Diagram, Plan, Plot, Bulldozer, Machine | Text: Inmate 7 | Inmate 5 | and 6 | Epstei

Page 84
photo
740 x 552
Objects: Clothing, Lifejacket, Vest, Accessories, Strap, Belt | Text: 2 3 4 56789 10.11 12 13 2 14 2

Page 85
photo
876 x 1233
No significant content detected

Page 93
diagram
2056 x 1165
Objects: Diagram, Dynamite, Weapon | Text: Lower Tiers | Upper Tiers | L Tier | M Tier | J Tier
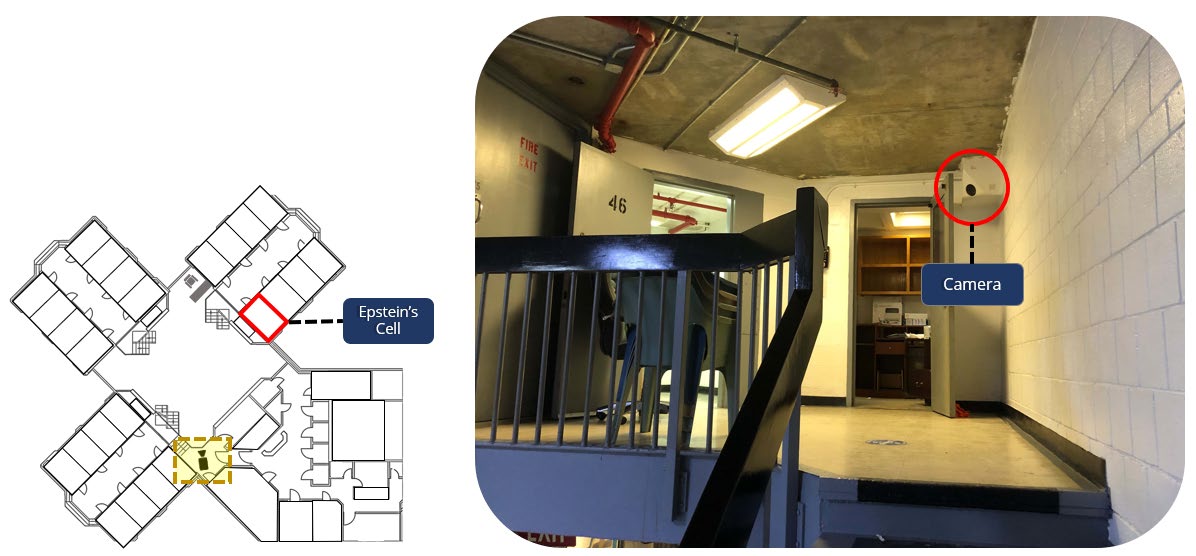
Page 94
property
1196 x 556
Objects: Architecture, Building, House, Housing, Staircase, Handrail, Hospital, Indoors | Text: FIRE

Page 95
photo
1367 x 559
Objects: Indoors, Outdoors | Text: 46 | Epstein's | Cell

Page 96
photo
1875 x 1154
Objects: Indoors, Outdoors | Text: Stairway to L Tier

Page 97
photo
1982 x 1220
Objects: Indoors, Outdoors, Computer Hardware, Electronics, Hardware, Monitor, Screen | Text: SHU Of

Page 98
property
2100 x 839
Objects: Indoors, Architecture, Building, Hospital | Text: FIRE | Epstein's | EXIT | Cell | 9th Floo
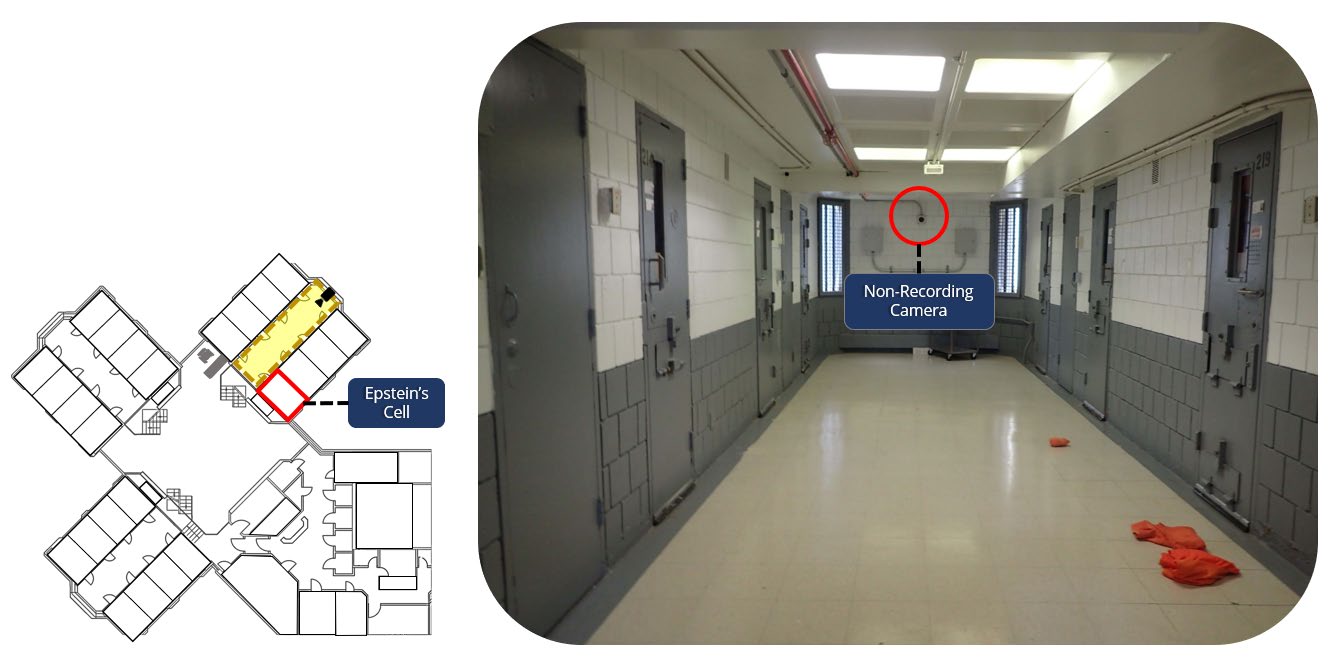
Page 99
property
1333 x 663
Objects: Architecture, Building, Corridor, Indoors, Hospital | Text: 219 | Non-Recording | Camera |

Page 122
document
1700 x 1975
Objects: Text, Document | Text: U. S. Department of Justice | Federal Bureau of Prisons | Central Of

Page 123
document
1700 x 2074
Objects: Page, Text, Letter | Text: OIG Official Draft Report: BOP's Care, Custody, and Supervision

Page 124
document
1700 x 1986
Objects: Page, Text, Letter | Text: OIG Official Draft Report: BOP's Care, Custody, and Supervision
- Activities Lieutenant (p.39) 5%
- Activities Lieutenant (p.58) 5%
- Activities Lieutenant (p.60) 5%
- Activities Lieutenant (p.61) 5%
- Activities Lieutenant (p.62) 5%
- Activities Lieutenant (p.63) 5%
- Activities Lieutenant (p.64) 5%
- Activities Lieutenant (p.74) 5%
- Activities Lieutenant (p.76) 5%
- Activities Lieutenant (p.107) 5%
- Activities Lieutenant (p.113) 5%
- Adequately Supervise (p.113) 50%
- Adequately Supervise (p.107) 50%
- Advanced Data (p.100) 25%
- After Action (p.51) 5%
- Aging Inmate (p.120) 95%
- Alert Notice (p.55) 50%
- Although Epstein (p.3) 5%
- Analysis Unit (p.27) 5%
- Analysis Unit (p.100) 5%
- ...and 659 more
- 3 Tiered St (p.33) address
- 4 Tiered St (p.34) address
- Adequately Supervise SHU Staff (p.107) location
- Adequately Supervise SHU Staff (p.113) location
- Associate Warden (p.39) location
- Belarus (p.66) location
- BOP (p.11) location
- BOP (p.40) location
- BOP (p.51) location
- BOP (p.105) location
- BOP documents (p.36) location
- BOP facilities are governed (p.15) location
- BOP institutions (p.11) location
- BOP Lieutenant training (p.119) location
- BOP policy governing inmates (p.17) location
- BOP Program Statement (p.16) location
- BOP records (p.4) location
- BOP records (p.36) location
- BOP records (p.37) location
- BOP records (p.38) location
- ...and 328 more
- File Path
- additional_files/2023.06 OIG Memorandum 23-085.pdf
- File Size
- 5,877 KB
- Processed
- 2025-12-20 18:45
- Status
- completed
-
BOP Epstein Records Part 1 of 4.pdf
Unknown - 1000 pages
21 shared people 8 shared places -
059.pdf
Unknown - 710 pages
14 shared people 11 shared places -
2020.11 DOJ Office of Professional Responsibility Report.pdf
Unknown - 348 pages
10 shared people 8 shared places -
074.pdf
Unknown - 338 pages
7 shared people 11 shared places -
Epstein Part 17 (Redacted).pdf
Unknown - 151 pages
5 shared people 12 shared places -
787-01.pdf
Unknown - 73 pages
4 shared people 13 shared places -
171.pdf
Unknown - 175 pages
7 shared people 9 shared places -
166.pdf
Unknown - 160 pages
7 shared people 7 shared places -
205.pdf
Unknown - 91 pages
6 shared people 8 shared places -
186-50.pdf
Unknown - 41 pages
4 shared people 10 shared places -
1078-5.pdf
Unknown - 161 pages
4 shared people 10 shared places -
153.pdf
Unknown - 94 pages
6 shared people 7 shared places -
146.pdf
Unknown - 92 pages
6 shared people 7 shared places -
363-11.pdf
Unknown - 40 pages
4 shared people 9 shared places -
795 (1).pdf
Unknown - 338 pages
5 shared people 6 shared places